Multiple Sclerosis
- is an autoimmune disease.
- Nongenetic trigger, such as a virus, metabolism, or environmental factors and Genetic factors together result in a self-sustaining autoimmune disorder that leads to recurrent immune attacks on the CNS – destruction of myelin
- The risk of MS relapse is reduced during pregnancy when compared with the pre-pregnancy period; however, the risk increases to greater than baseline in the first six months postpartum. Breastfeeding may slightly reduce this rate
| Early clinical and imaging features affecting prognosis in multiple sclerosis | |
| Better prognosis | Poor prognosis |
| Optic neuritis or isolated sensory symptoms as the initial presentation Complete recovery from the first neurological episode Long interval to second relapse No disability after five years Normal initial MRI Older age at disease onset | High relapse rate in first 2–5 years Substantial disability after five years Abnormal initial MRI with large lesion load Infratentorial or spinal lesions on MRI |
epidemiology
- F>M incidence – two to three times as many women as men
- onset is usually between 16 and 50 years with a peak between 20-40 years
- 15% of sufferers of the disease have a blood relative with MS
- 85% of MS have RRMS at onset, of which 66% may develop secondary progressive MS MS:
- 15% of MS hsd primary progressive MS where symptoms gradually develop and worsen over time from the start, without ever experiencing relapses and remissions
- 5% of males and females with MS are aged between 40 and 74 years of age
Risk Factors
- Race: White > Black
- Gender: Female > Male (2:1)
- High socioeconomic status
- Northern latitudes
- Environmental factors (toxins, viruses)
- Infectious Mononucleosis
- Tobacco Abuse
- HLA histocompatible Antigens
- Vitamin D Deficiency (or less sunlight exposure)
Symptoms
- sensory deficits:
- Sensory loss of vibration, proprioception or nociception (37%)
- Paresthesias with numbness or tingling Sensation (24%)
- Lhermitte Sign (3%) – Electrical Sensation down spine on neck flexion
- Optic Neuritis (36%) – inflammation, degeneration, or demyelination of the optic nerve
- usually unilateral
- rarely bilateral
- upper motor neurone deficit:
- most commonly a spastic weakness of the legs
- Diplopia (15%)
- cerebellar damage:
- Ataxia or Incoordination (11%)
- dysarthria
- nystagmus
- Vertigo (6%)
- Urinary Incontinence (4%)
- Dementia (2%)
- Cognitive dysfunction is a late disease finding (consider alternative diagnosis if a concern at presentation)
- Findings may include Learning Difficulty, memory deficit, slowed processing speed
- Visual Loss (2%)
- Facial palsy (1%)
- Erectile Dysfunction or Sexual Dysfunction (1%)
- Seizures (1%)
- psychiatry: anxiety, depression, behavioral dist, cognitive impairment
- Other findings
- Fatigue
- Hearing Loss or Tinnitus
- Heat intolerance
Signs
- Dysarthria
- Decreased pain, vibration and position sense
- Decreased coordination and balance
- Ataxia
- Difficult Tandem Walking
- Eye Exam
- Visual Field Defects
- Decreased Visual Acuity
- Red color Perception
- Afferent Pupillary Defect
- Optic Nerve pallor (Optic Neuritis)
- Nystagmus (most commonly Horizontal Nystagmus)
- Bilateral Internuclear Ophthalmoplegia
- Nystagmus of abducting eye on lateral gaze
- Other eye with slow adduction
- Reflexes
- Deep Tendon Reflexes hyperactive
- Spasticity
- Abdominal reflexes lost
- Ankle Clonus present
- Babinski Reflex with up-going toes
- Charcot’s Triad
- Intention Tremor
- Nystagmus
- Scanning speech
- Hot Bath Test
- Hot bath exacerbates visual signs
| Common sites, signs and symptoms of clinically isolated syndrome or multiple sclerosis relapses1 | |||
| Site | Condition | Symptoms | Signs |
| Optic nerve | Optic neuritis | Pain on eye movement, blurred vision | Reduced monocular visual acuity, colour desaturation Fundoscopy may be normal or may show a swollen optic disc |
| Cerebrum | Focal supratentorial syndrome | Dependent on cerebral location (eg hemianopia in an appropriately located occipital lesion) | |
| Cerebellum | Cerebellar disease | Unsteadiness | Limb or gait ataxia; horizontal or torsional gaze-evoked nystagmus |
| Spinal cord (usually multifocal and asymmetric) | Partial myelitis affecting pyramidal tracts | Upper or lower limb weakness | Pyramidal distribution weakness |
| Partial myelitis affecting spinothalamic, posterior columns | Unilateral or bilateral limb numbness or paraesthesias; Lhermitte’s phenomenon | Sensory level | |
| Any spinal cord lesion | Urinary frequency or urge incontinence, constipation erectile dysfunction | ||
| Brainstem – medial longitudinal fasciculus | Internuclear ophthalmoplegia | Blurred or double vision | Internuclear ophthalmoplegia |
| Brainstem – pyramidal tracts, spinothalamic and posterior columns | Similar to that described in spinal cord | ||
TYPES
| Clinically Isolated Syndrome (CIS) | first episode of neurologic symptoms caused by inflammation and demyelination in the CNS = Vision problems (optic neuritis) = Vertigo = Loss of sensation in the face = Weakness in the arms and legs, with one side of the body affected more than the other = Difficulty with coordination, balance, walking, speaking and swallowing (ataxia) = Bladder problems l= east 24 hours A person with CIS has a high likelihood of a second episode of neurologic symptoms and a diagnosis of relapsing-remitting MS if an MRI (magnetic resonance imaging) shows brain lesions that are similar to those seen in MS. Without those lesions, the likelihood of an MS diagnosis is much lower | |
| Relapsing remitting | Approximately 85% of people with MS are initially diagnosed with RRMS Relapse: periods when symptoms flare up aggressively Remission: followed by periods of some or complete recovery, disease does not progress.followed by periods of partial or complete recovery, or remission. Active: relapses and/or evidence of new MRI activity over a specified period of time or not active worsening :confirmed increase in disability following a relapse) or not worsening. | 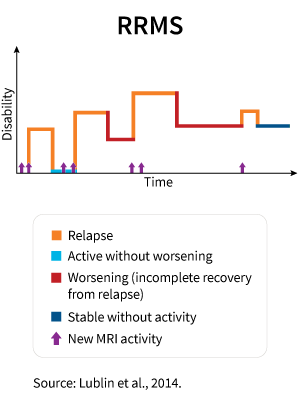 |
| Primary progressive | With PPMS, neurologic function worsens or disability accumulates as soon as symptoms appear, without early relapses or remissions. PPMS can be further characterized as either active : with an occasional relapse and/or evidence of new MRI activity over a specified period of time or not active with progression: evidence of disability accrual over time, with or without relapse or new MRI activity) or without progression. Approximately 15% of people with MS are diagnosed with PPMS. | 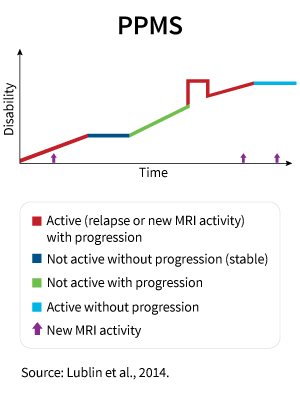 |
| Secondary progressive | SPMS follows the initial relapsing-remitting course. Some people diagnosed with RRMS eventually go on to have a secondary progressive course, in which neurologic function worsens progressively or disability accumulates over time. SPMS can be further characterized as either active : with relapses and/or evidence of new MRI activity during a specified period of time) or not active with progression: evidence of disability accrual over time, with or without relapses or new MRI activity) or without progression. | 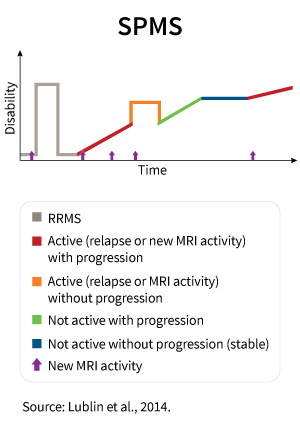 |
| Radiologically isolated syndrome (RIS) | Lesions on the brain or spinal cord — not explained by another diagnosis — consistent with lesions of MS andNo past or current neurological symptoms or abnormalities found on a neurological exam |
Classifying MS
- active/not active
- worsening/stable
- with progression/without progression.
- Active or not active is used in all types of MS to describe whether or not you’re having relapses and/or if new lesions can be seen on an MRI scan. For instance, if you have RRMS and you’re experiencing relapses, your MS would be considered active. Alternatively if you have PPMS and no new lesions could be seen on an MRI scan, your MS would be termed not active.
- Worsening or stable is used in people with RRMS to describe whether your disability is increasing or staying at the same level following a relapse.
- With progression or without progression is used in people with PPMS and SPMS to describe whether your level of disability is increasing or staying the same over a period of time.
- The committee also suggested that clinically isolated syndrome (CIS), someone’s first episode of neurological symptoms, be classed as a type of MS. By noting CIS as the potential first sign of MS, people with CIS can get access to treatment and advice. Early treatment is understood to be important in reducing the impact of MS over the course of a person’s lifetime.
DIAGNOSIS
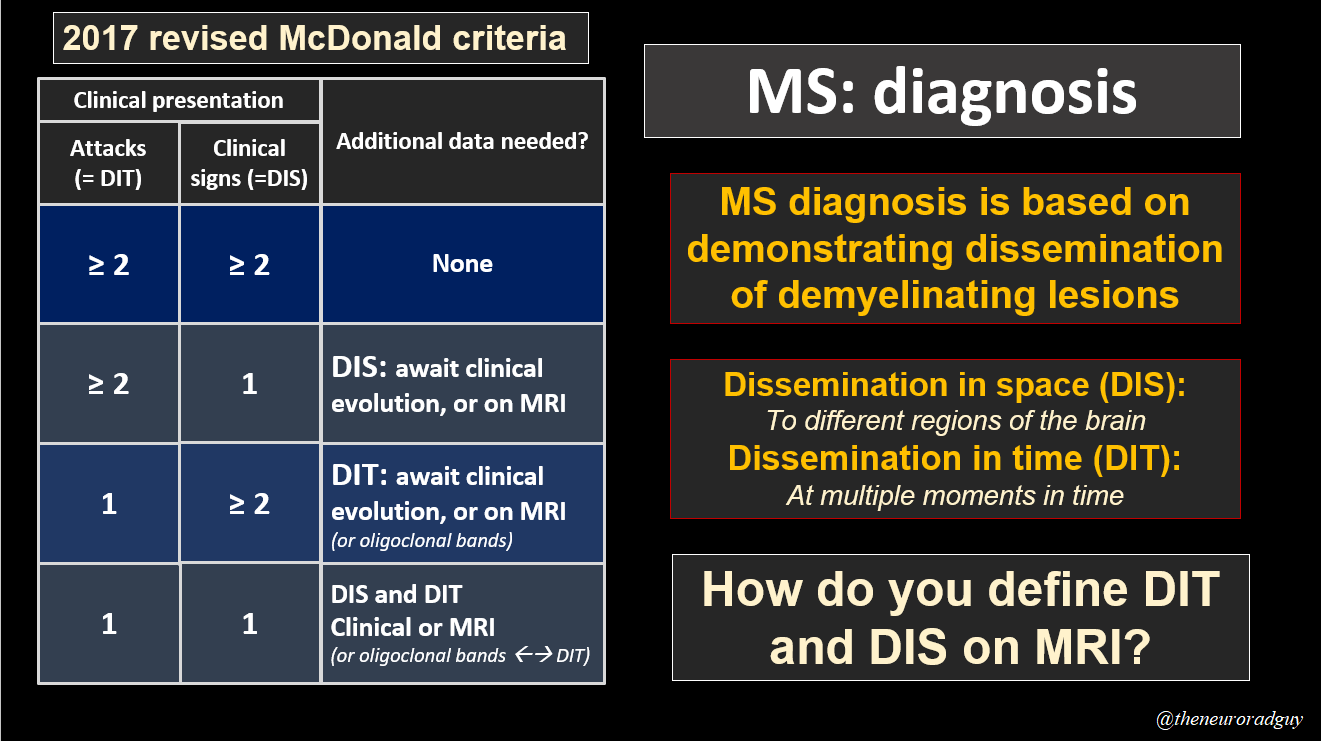
McDonald criteria “multiple in time and multiple in space”
Do not diagnose MS on the basis of MRI findings alone
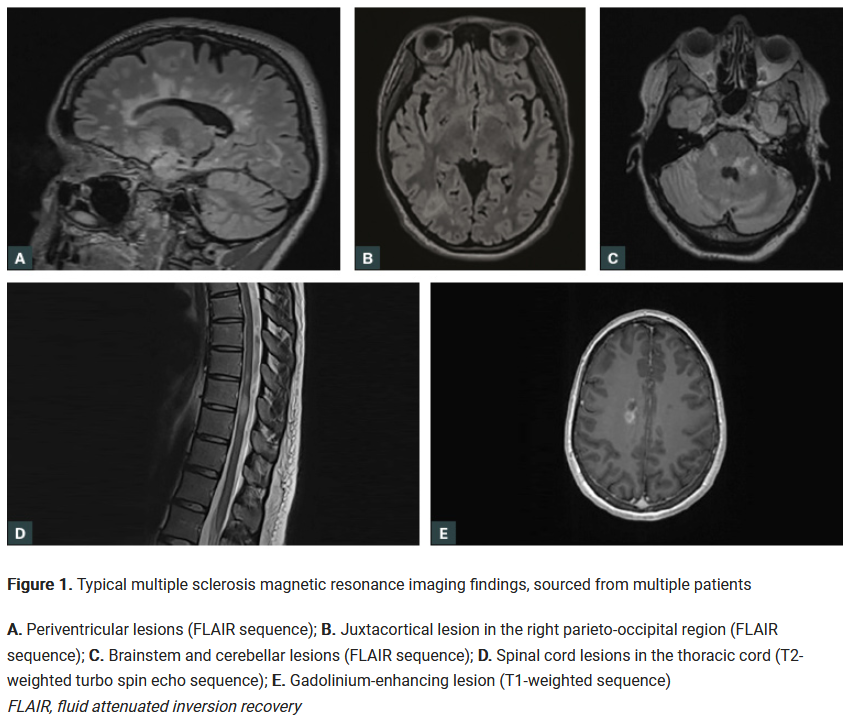
- MRI – white matter lesions of demyelination
- CSF – oligoclonal bands (additional immunoglobulins)
DDx
- Epilepsy
- TIA, Stroke
- SLE
- HIV, Toxo
- Sarcoid
- Neoplasm
Management:
- General Supportive Measures
- Keep Cool
- Regular Exercise
- Pursuit of wellness and positive attitude
- Education regarding the disease
- Support from family and MS support groups
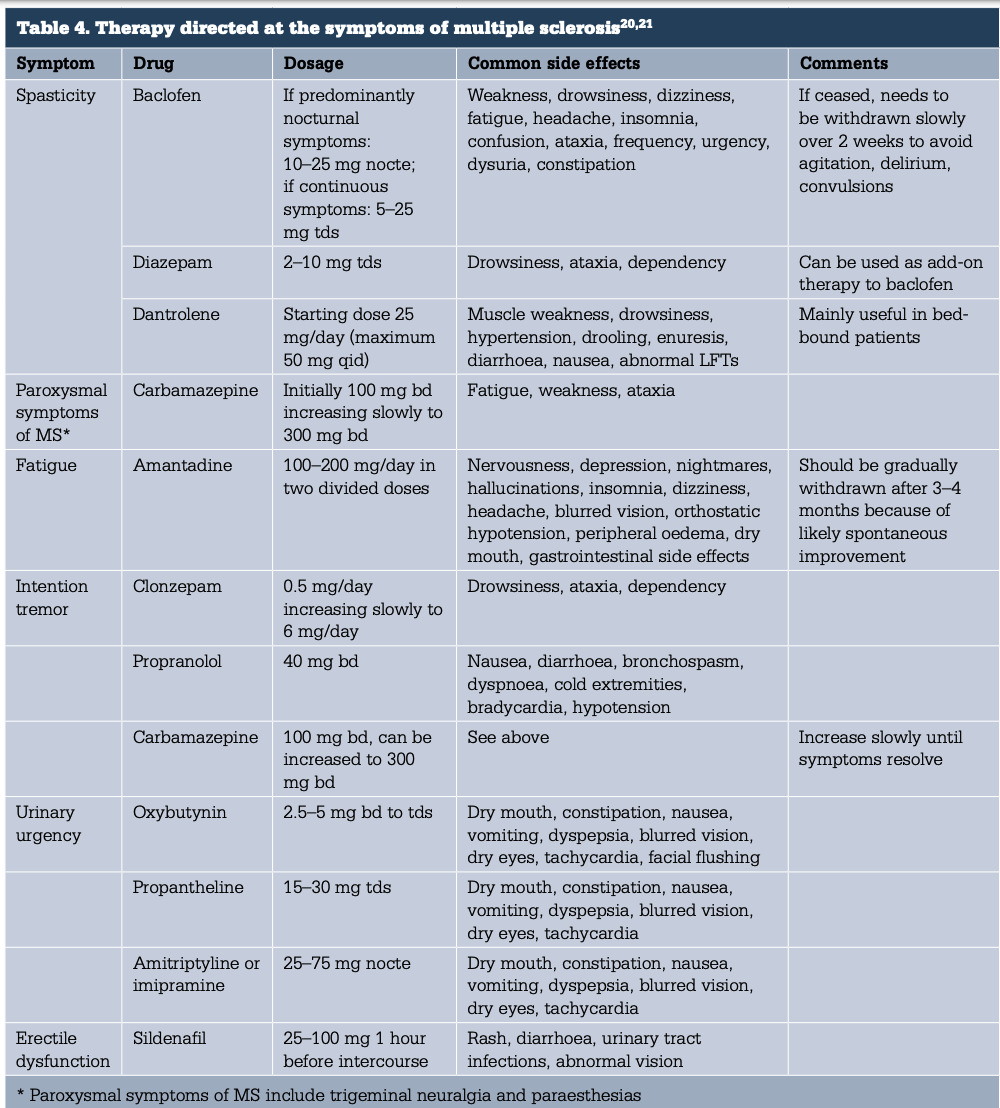
- spasticity
- physiotherapy
- baclofen
- gabapentin
- increase the dose gradually in at least 2-week increments to optimise symptom improvement or until they reach the maximum dose they can tolerate
- stop taking the medicine if there is no benefit at the maximum tolerated dose
- oscillopsia
- is a symptom of jumbling eye movements, manifested as blurred vision when walking or running, and is caused by poor stabilization of the retinal image during head movement
- consider gabapentin as a first-line
- is a symptom of jumbling eye movements, manifested as blurred vision when walking or running, and is caused by poor stabilization of the retinal image during head movement
- urinary frequency and incontinence:
- anti-cholinergics:
- oxybutynin hydrochloride
- tricyclic antidepressants e.g. amitriptyline
- intermittent self-catheterisation
- anti-cholinergics:
- bowel symptoms:
- stool softeners
- high roughage diet
- impotence:
- intracavernosal injection of papaverine
- sildenafil
- paroxysmal episodes of altered sensation:
- anti-convulsants
- seizures – anti-convulsants
- cerbellar tremor:
- is a lack of evidence for pharmacological management of ataxia and tremor in people with MS
- depression:
- fatigue:
- non-pharmacological management of mobility problems and fatigue
- vestibular rehabilitation
- supervised exercise programmes
- progressive resistance training
- aerobic exercise
- amantadine
- amantadine 100 mg bd helps 40% of patients
- offer amantadine to treat fatigue in people with MS
- modafinil
- selective serotonin reuptake inhibitor (SSRI)
- non-pharmacological management of mobility problems and fatigue
Acute relapses
- Differentiate relapse from pseudorelapse
- infection, psychosomatic, heightened body awareness
- Repeat MRI only indicated if doubt of cause or change of meds.
- Mild – rest, reassure
- Moderate – unpleasant symptoms and disability 🡪 Prednisone PO
- Severe – severe symptoms like optic neuritis, paraplegia, brainstem 🡪 admit, Methylpred IV, MDT rehab
- Non-resolving relapse 🡪 plasmapheresis
Chronic meds
Immune modulator , Immunotherapy or Immunosuppression