TIA
- is defined as “rapidly developed clinical signs of focal or global disturbance of cerebral function lasting fewer than 24 hours, with no apparent non-vascular cause”.
- The lifetime risk of stroke is:
- in 5 for women
- 1 in 6 for men
- The risk of stroke following TIA is high
- up to 1 in every 5 patients go on to have a stroke in the first 3 months
- half the risk within the first few days.
- New evidence demonstrates aggressive, early management can reduce the incidence of stroke by up to 80%
- The traditional definition of TIA involves an arbitrary time cut off of 24 hours, in reality most attacks last approximately 20 minutes.
- Some authorities internationally have called for a revised definition in which the duration of symptoms is 1 hour or less.
History
- Nature – was the deficit of the motor, somatosensory, visual and/or other system?
- Quality – was there a loss of function (e.g. weakness or numbness) or gain of function (e.g. jerking, parasthesia)?
- Anatomical distribution – did the deficit involve the face, arm or leg; or face, arm and leg?
- Onset – was it sudden, stuttering or gradual?
- Evolution – e.g. did the deficit recover, stabilise or progress?
neurological examination
- Visual fields
- Plantars, reflexes and eye movements
- Speech, visual fields, eye movements, facial weakness, limb weakness & plantars
- Cranial nerves and sensory examination
Risk factor assessment and stratification
- ABCD2 – high risk of stroke within the first 7 days of TIA
- A = AGE
>60 years (1 point)
- B = BLOOD PRESSURE
>140mmHg systolic ± =90mmHg diastolic (1 point)
- C = CLINICAL FEATURES:
unilateral weakness (2 points)
speech impairment without weakness (1 point)
- D = DURATION
60mins (2 points)
10-59 mins (1 point)
- D = DIABETES (1 point)
- Interpretation: >4 = HIGH risk; <4 = LOW risk2
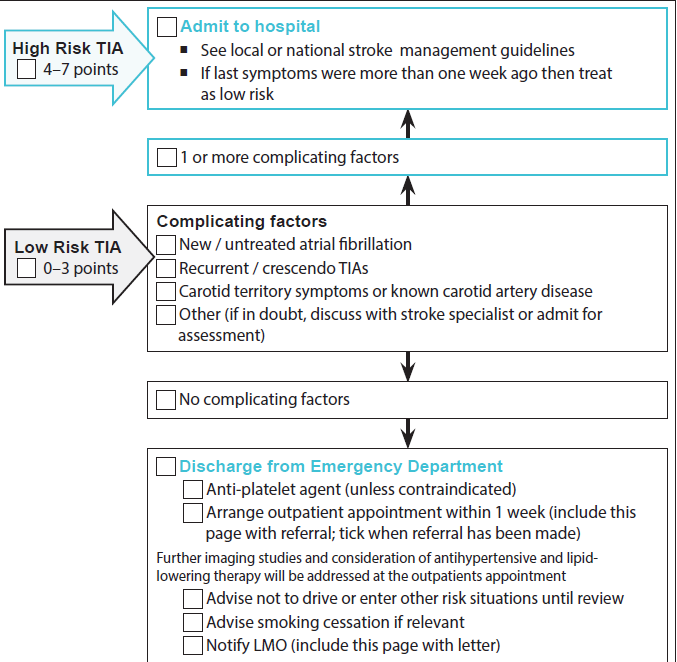
- high risk patients – Patients with ABCD2 >4
- Urgent CT brain
- Carotid duplex ultrasound
- should be admitted to a stroke unit
- where specialist assessment can be carried out urgently
- low risk patients – Patients with ABCD2 <4
- may be managed in the community, by a GP, private specialist or where possible referred to a specialist TIA clinic
- CT scan and carotid ultrasound (where indicated) as soon as possible (ie. within 48-72 hours)
- seen within 7-10 days
- Ideally the sooner the patient is seen and commenced on therapy the lower the risk of subsequent events.
Acute management of TIA

- Treat AF with anticoagulation – after excluding haemorrhage (INR 2.5)
- Minor stroke deficit which is rapidly improving, such is the case with TIA, is a contraindication to intravenous rtPA
Carotid Endarterectomy : Indication
- Carotid stenosis >70% ICA – stenosis in symptomatic TIA or CVA patients -> incidence of death or major CVA = 2-5%
- Carotid stenosis 50-69% ICA – CEA should only be considered where the benefits clearly outweigh potential harms.
- Eligible patients should undergo CEA within 2 weeks
- CEA is not recommended for those with <50% symptomatic stenosis or those with <60% asymptomatic stenosis
Secondary prevention
- Treat hypertension if > 140/90
- Antiplatelet therapy as above
- Blood pressure lowering agents
- Using an ACE inhibitor alone or with a diuretic
- High potency statin – regardless lipids
- Behaviour change (e.g. smoking, diet, exercise, alcohol consumption)
- Lifescripts program is a national initiative which provides tools for
- TIA should not drive 2 weeks, 4 weeks if commercial
*In the PROGRESS trial, combination therapy with perindopril plus indapamide reduced stroke risk by 43% in hypertensive and non-hypertensive patients with a history of stroke or TIA.
metro GPs – Barriers/Potential solutions
- Unaware of local stroke units and protocols
- Establish networks with local neurologists and stroke units
- Direct communication between referring and receiving clinicians is essential to smooth transitions
- Develop formal bypass or diversion protocols so that individuals who meet inclusion criteria for time-dependant therapy have an opportunity to receive them
- Lack of tools/ resources
- Become involved in care pathway planning for patients with TIA and stroke
- Use pre-hospital screening tools such as ABCD2
- Contact the National Stroke Foundation for additional information
rural GPs – Barriers/Potential solutions
- Rural centre – No CT on site
- Develop internal protocol to transfer patient with suspected TIA to local private hospital with CT capabilities
- Develop bypass or diversion protocols with local ambulance service
- Conduct training of ambulance staff for rapid assessment of signs of TIA/stroke and transfer protocols
- No neurologist or experienced technician on site
- Develop agreements with local private hospitals for CT scan interpretation or reporting
- Support future training of local staff with CT imaging and interpretation Telehealth protocols
Driving after Transient ischaemic attack (advisory only)
Private standards
- A person should not drive for at least 2 weeks following a TIA.
- A conditional licence is not required