Hypokalaemia
Hypokalaemia is defined as a serum potassium level of < 3.5 mmol/L. ECG changes generally do not manifest until there is a moderate degree of hypokalaemia (2.5-2.9 mmol/L). The earliest ECG manifestation of hypokalaemia is a decrease in T wave amplitude.
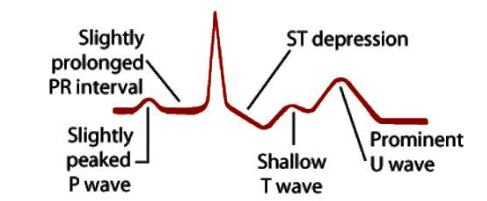
ECG features of hypokalaemia (K < 2.7 mmol/L)
- Increased P wave amplitude
- Prolongation of PR interval
- Widespread ST depression and T wave flattening/inversion
- Prominent U waves (best seen in the precordial leads V2-V3)
- Apparent long QT interval due to fusion of T and U waves (= long QU interval)
With worsening hypokalaemia…
- Frequent supraventricular and ventricular ectopics
- Supraventricular tachyarrhythmias: AF, atrial flutter, atrial tachycardia
- Potential to develop life-threatening ventricular arrhythmias, e.g. VT, VF and Torsades de Pointes
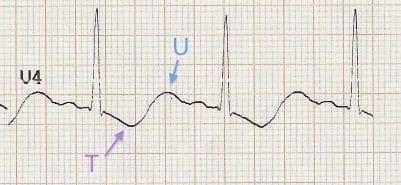
Hypokalaemia: T wave inversion and prominent U waves
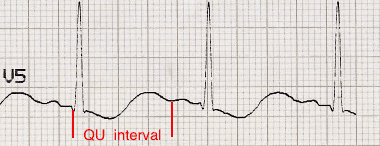
QU interval: The apparent pseudo-prolonged QT interval is actually the QU interval with an absent T wave
| Degree of hypokalaemia | Potassium level (mmol/L) |
| Mild | 3.0 – 3.4 |
| Moderate | 2.5 – 2.9 |
| Severe | ≤ 2.4 |
- Hypokalaemia is often associated with hypomagnesaemia, which increases the risk of malignant ventricular arrhythmias
- Check both potassium and magnesium levels in any patient with an arrhythmia
- Replace potassium to ≥ 4.0 mmol/L and magnesium to ≥ 1.0 mmol/L to stabilise the myocardium and protect against arrhythmias – this is standard practice in most CCUs and ICUs
ECG Examples
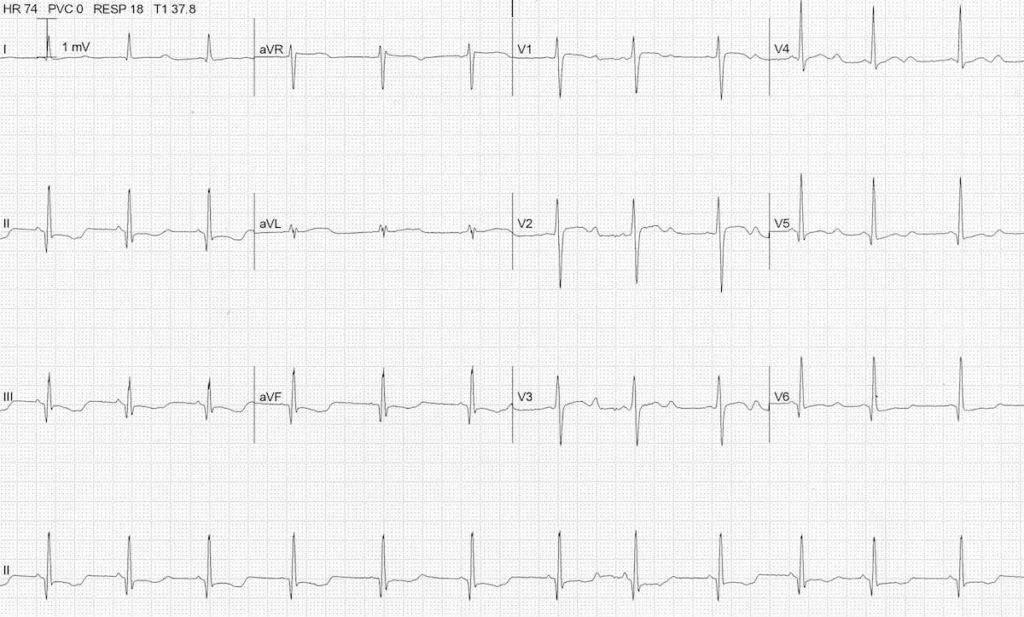
Example 1
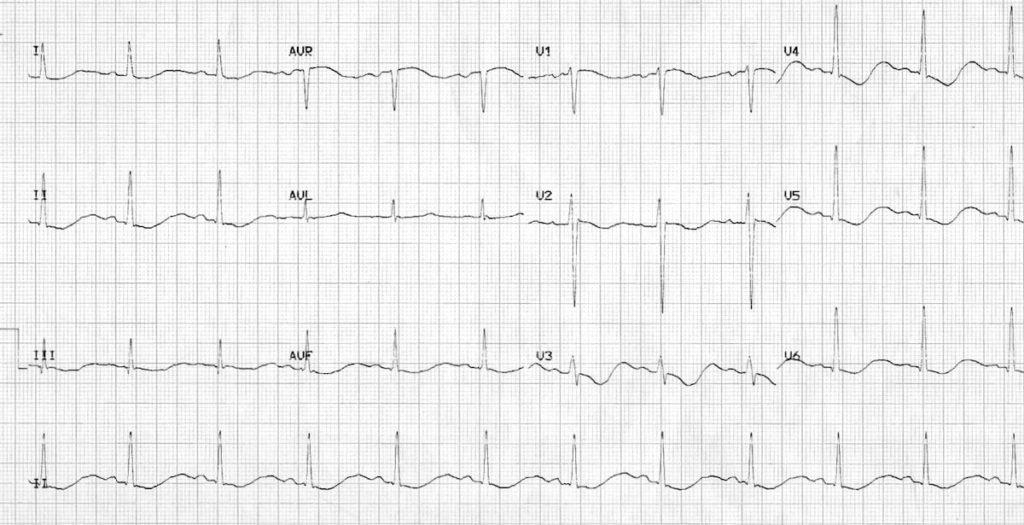
Hypokalaemia: Widespread ST depression and T wave inversion, Prominent U waves
Long QU interval, This patient had a serum K+ of 1.7
Example 2
Hypokalaemia
ST depression and T wave inversion best noted in inferior leads , Prominent U waves, Long QU interval, The serum K+ was 1.9 mmol/L.
Example 3
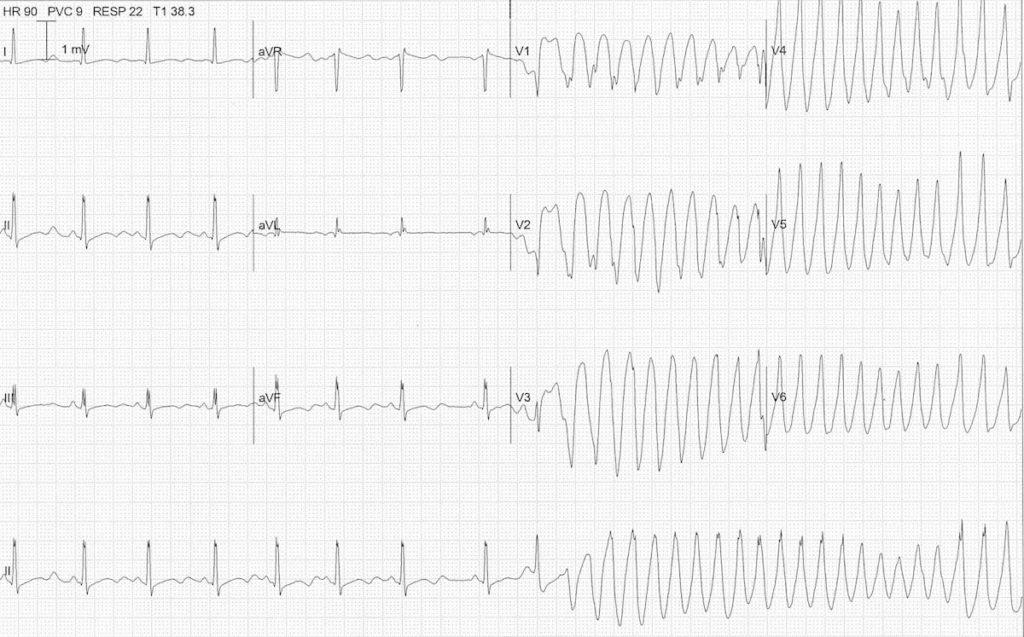
Hypokalaemia causing Torsades de Pointes, Another ECG from the same patient
Note the atrial ectopic causing ‘R on T’ (or is it ‘R on U’?) that initiates the paroxysm of TdP
Treatment
Moderate to severe or symptomatic hypercalcaemia (e.g. lethargy, coma, ECG
changes [shortened QT interval])
- Rehydration – intravenous sodium chloride 0.9%. Volume infused should be sufficient
to maintain a urine output greater than 60 mL/hr. Seek senior advice. - Bisphosphonate therapy with either zoledronic acid or pamidronate may be indicated.
Seek senior advice.
Long-term management
- Review for possible causes including diet or supplements (vitamin D or calcium),
sarcoidosis and other granulomatous disease; drug causes such as calcitriol excess
or thiazide diuretics, and hypercalcaemia due to spinal cord injury and/or immobility