Travellers’ diarrhea
- 20% to 60% attack rates for a 2‐week stay
- Duration of illness usually 4 days
- Interferes with travel plans – 30-60%
- 3.0% of patients with TD developed Irritable Bowel Syndrome within 6 months of travel cf 0.7% without TD.
- Most often bacterial – Escherichia coli (ETEC), Other – shigella, campylobacter, salmonella, Also norovius, protozoal parasites
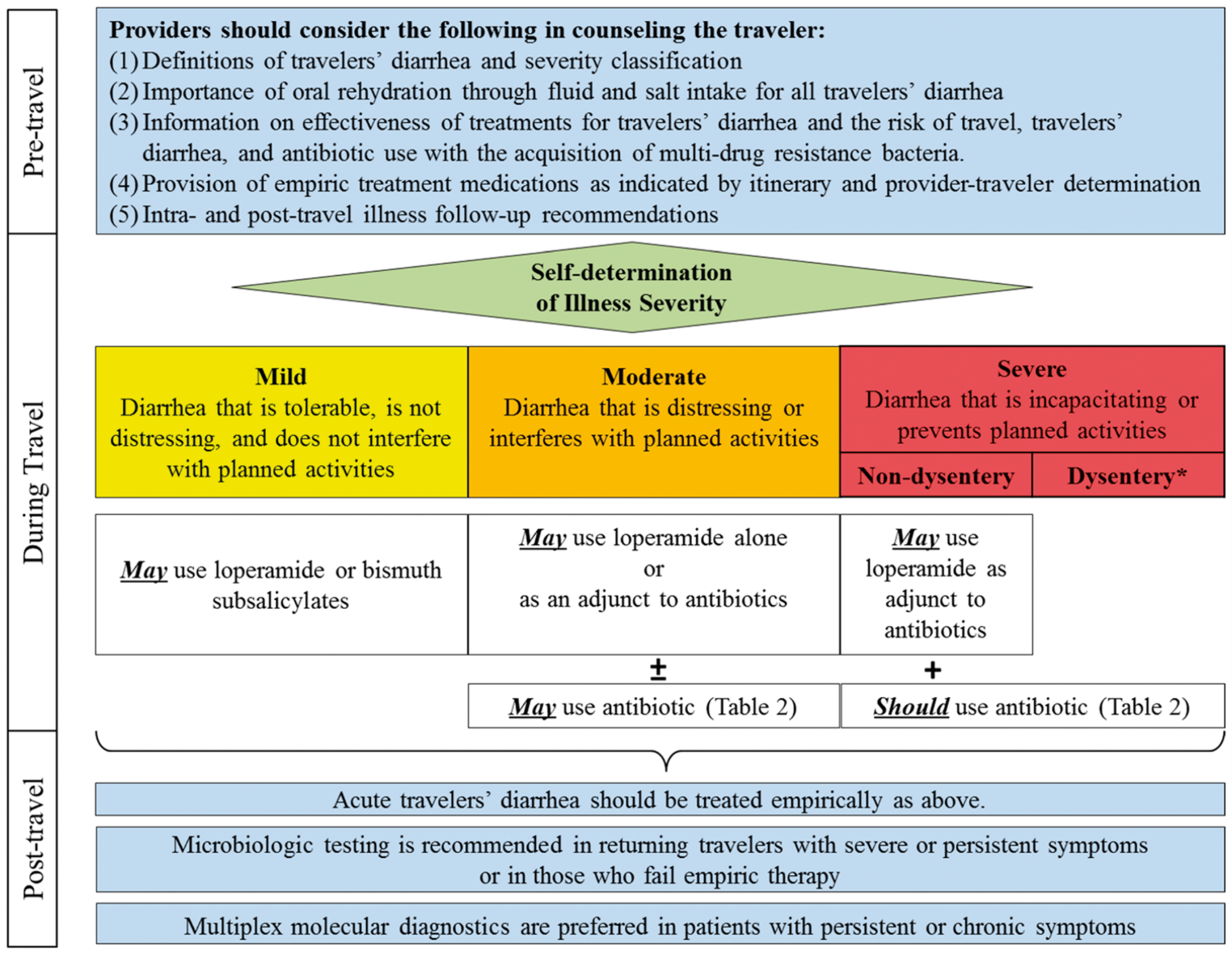
Treatment
Goal of treatment = prevention and treatment of dehydration
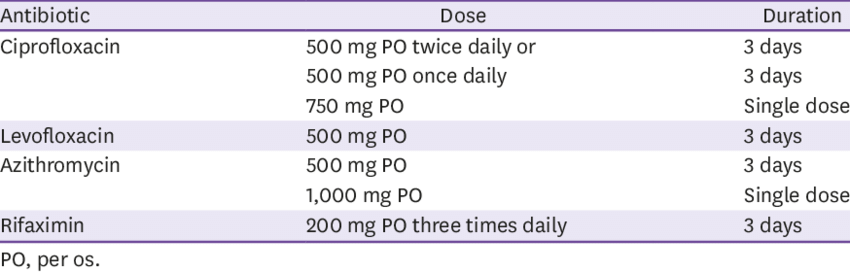
Antibiotic Options
- Azithromycin
- preferred to treat severe TD
- suitable for: All age groups, including children and pregnant women.
- in Asia (particularly South and South-East Asia) most common cause – Campylobacter high degree of resistance to fluoroquinolones (such as Norfloxacin or Ciprofloxacin)
- Single dose: 1 g for adults, 20 mg/kg for children (up to 1 g)
- Extended treatment (if persistant Symptoms): 500 mg daily for 2 days, 10 mg/kg for children (up to 500 mg)
- preferred to treat severe TD
- Norfloxacin
- Single dose: 800 mg for adults, 20 mg/kg for children (up to 800 mg)
- Extended treatment (if needed): 400 mg every 12 hours for 2 days, 10 mg/kg for children (up to 400 mg)
- Note: Not recommended for routine use in pediatric patients due to potential adverse effects on developing cartilage. Use in children only when no alternatives are available and the benefits outweigh risks.
- Note: No oral liquid formulation available.
- Ciprofloxacin
- Single dose: 750 mg for adults, 20 mg/kg for children (up to 750 mg)
- Extended treatment (if needed): 500 mg every 12 hours for 2 days, 12.5 mg/kg for children (up to 500 mg)
- Notes: Like norfloxacin, concerns exist regarding cartilage development in children. No oral liquid formulation available
- seek medical therapy
- frank blood in the stool
- unremitting fevers (>38.5°C for 48 hours)
OTHER
- Loperamide
- can be used in adults without fever/bloody stools to reduce stool frequency and improve comfort.
- may be combined with Antibiotic regimens
- 4 mg first dose, then
- 2 mg dose after each loose stool
- not to exceed 16 mg in a 24 hour period.
- Avoid loperamide if very severe e.g. bloody
- Tinidazole
- for suspected protozoan infections(ie: Giardia intestinalis) if initial treatments fail (TD persists following the 3-day course of antibiotic therapy )
- dose of 2 g (4 x 500 mg tablets)
Diarrhea Children
- Main Treatment Strategy:
- Oral rehydration solution (ORS) is the cornerstone of therapy, especially crucial for children under 6 years of age.
- Antibiotic Treatment:
- Azithromycin
- Azithromycin 20mg/kg for up to 3 days
- Fluoroquinolones (such as ciprofloxacin or norfloxacin at 10 mg/kg twice daily) can be considered if azithromycin is unsuitable.
- Concerns about their impact on cartilage growth in children have not been supported by recent research, making them a viable alternative – reference – unclear (https://www.racgp.org.au/afp/2015/january-february/advising-travellers-about-management-of-travellers#ref-22 : Yung A, Leder K, Torresi J, et al. Manual of Travel Medicine. 3rd edn. Melbourne: IP Communciations, 2011. Search PubMed,)
- Azithromycin
- DON’T give Loperamide
- US guidelines infants <2 years of age
- UK guidelines <4 years
- Australian guidelines state <12 years
- Antimotility medications like loperamide are contraindicated in children due to risks such as
- paralytic ileus
- toxic megacolon
- drowsiness. (narcotic effect)
- Probiotics and Prebiotics
- Cochrane review found insufficient evidence to recommend it
- Insufficient evidence
Prevention
- Precautions: Opt for hot, freshly cooked foods, peelable fruits, and beverages that are bottled or boiled.
- Commercial packets of oral rehydration salts are readily available in pharmacies and should be purchased before travel.
- Avoidance: raw or undercooked food (particularly meat or seafood), fresh salads, peeled fruit, unpasteurised milk or milk products, unboiled water, and ice. Foods sold by roadside vendors often pose the greatest infection risk.
- Antimicrobial prophylaxis:
- Generally not recommended due to the risk of developing resistance; consider for immunocompromised travelers for no more than three weeks.
- Rifaximin – shown to be effective and is approved for use for TD prevention in some countries, but it is not approved for this indication in Australia
- Immunization: Limited role but includes vaccines like rotavirus (infants) and cholera vaccine.
- cholera vaccine has >90% efficacy for prevention of Vibrio cholera but travellers are rarely at risk of infection with this pathogen
- vaccine contains a recombinant B subunit of the cholera toxin that is antigenically similar to the heat-labile toxin of ETEC; therefore, the cholera vaccine may also reduce ETEC TD = However, it is not licensed for TD prevention in Australia
- Non-antibiotic interventions: Probiotics and other agents like bovine colostrum have limited effectiveness.