Dermatitis
- Dermatitis refers to a group of itchy inflammatory conditions characterized by epidermal changes.
- The terms dermatitis and eczema are often used interchangeably.
Relationship with Eczema:
- ALL eczema is a dermatitis
- BUT not all dermatitis is eczema.
- Dermatitis = any cause of skin inflammation affecting the epidermis.
- Eczema = derived from the Greek word for “to boil or bubble over”, which pathologically manifests as oedema within the epidermis (called spongiosis).
Classification:
Dermatitis can be categorized based on various factors:
- Cause:
- Allergic contact dermatitis
- Photosensitive dermatitis
- Clinical Appearance:
- Discoid dermatitis/Nummular dermatitis
- characterized by coin-shaped patches of irritated skin.
- It often occurs after skin injuries, such as insect bites or abrasions, and tends to be more prevalent in winter.
- Hyperkeratotic dermatitis
- Pompholyx/Dyshidrotic eczema
- primarily affects the palms of the hands and soles of the feet.
- It is characterized by small, itchy blisters and can be triggered by factors like stress or exposure to certain metals.
- Discoid dermatitis/Nummular dermatitis
- Site of Predilection:
- Hand dermatitis
- Eyelid dermatitis
- Lower leg dermatitis
- Combined Factors:
- Various factors may act as triggers together (allergic, irritant, and endogenous factors).
Epidemiology of Dermatitis
- Dermatitis is common, affecting about one in every five persons at some stage in their life.
- Different types are more frequent at different life stages.
- Atopic dermatitis and pityriasis alba are more common in children
- Hand eczema is more common in young and middle-aged adults
- Venous or gravitational eczema, asteatotic dermatitis, and nummular eczema are more common in middle and older age groups.
Clinical Features of Dermatitis
- Dermatitis may be acute or chronic, with varying appearances.
- Acute dermatitis shows
- redness
- swelling
- vesiculation
- oozing.
- Chronic eczema presents with
- skin thickening
- hyperkeratosis
- excoriation.
Racial Variation in Clinical Features
- Redness may be more challenging to appreciate in darker skin types.
- Post-inflammatory hypo- and hyperpigmentation are more frequent in darker skin types.
Types of Dermatitis and Their Causes
Exogenous Dermatitis:
- Allergic contact dermatitis — due to immune sensitisation of an individual to an allergen, often at even low concentration, such as nickel, hair dye, rubber, or perfumes; identified by patch testing.
- Irritant contact dermatitis — will occur in anyone exposed to an irritant at sufficient concentration for long enough; irritants include soaps, detergents, organic solvents, degreasing agents, abrasives, desiccants, dust, urine, and even water
- Photosensitive dermatitis — triggered by light or UV radiation
- Post-traumatic dermatitis — due to physical injuries such as abrasions, burns, or surgery (eg, autonomic denervation dermatitis)
- Dermatitis induced by local skin infections such as bacterial, fungal, and viral e.g. molluscum contagiosum and HTLV-1 disease
- Drug-induced dermatitis.
Endogenous Dermatitis:
| Atopic dermatitis — a common form of dermatitis occurring in children and adults, and often occurring in families with a background of asthma and hay fever | |
| Seborrhoeic dermatitis — common chronic eczema affecting the face, scalp, ears and major flexures, due to a reaction to yeasts that colonise the skin |  |
| Discoid (nummular) dermatitis — coin-shaped patches of dermatitis usually affecting the limbs |  |
| Lichen simplex — chronic dermatitis that thickens due to perpetual scratching | |
| Pityriasis alba — pale patches of dermatitis affecting the cheeks | |
| Hand dermatitis — internal, external irritants and allergic factors may all play a part even in a single individual | |
| Eyelid dermatitis — again, often of mixed cause | |
| Otitis externa — dermatitis affecting the ear canal and the pinna | |
| Venous or gravitational dermatitis — dermatitis due to malfunction of the lower leg vein valves | |
| Juvenile plantar dermatitis — a glazed and fissured forefoot eczema occurring in children | |
| Metabolic dermatitis — seen in – obesity – hypertension – dyslipidaemia – insulin resistance. | |
| Chronic superficial scaly dermatitis — finger-shaped patches of eczema occurring on the trunk | |
| Asteatotic dermatitis — crazy-paving shaped dermatitis due to degreasing of the skin from excessive bathing and soap use on the legs in the elderly | |
| Halo dermatitis or Meyerson naevus — this can surround a benign mole | |
| Erythrodermic dermatitis — severe dermatitis when more than 80% of the skin is affected. |
Differential Diagnosis of Dermatitis
- Bacterial and fungal infections
- Connective tissue diseases
- Rosacea
- Blistering diseases
- Skin tumors
- Cutaneous T-cell lymphoma
Investigation and Treatment of Dermatitis
Investigation:
- Detailed history and examination
- Skin scraping
- swab
- patch testing
- light testing
- skin biopsy
- blood tests
Treatment:
- General Principles:
- Allergen and irritant identification and avoidance
- Personal protective equipment for specific cases
- Exacerbated by heat, prickle (wool, nylon, seams, labels) and dryness
- Avoid triggers:
- Avoid soap
- Avoid hot baths
- Avoid “prickly” clothes
- Avoid scratching
- Moisturisers:
- Dermeze (50% soft/ 50% liquid paraffin oil)
- 4-6x a day if needed
- Applied over CS if using
- Topical Therapies:
- Emollients, potassium permanganate soaks, paste bandages
- topical steroids
- Hydrocortisone 0.5-1% on face BD
- Elocon on body OD
- Calcineurin inhibitors, JAK inhibitors’
- Physical Therapies:
- Ultraviolet B and Psoralens UVA (PUVA)
- Systemic Agents:
- Antihistamines (for itch)
- antibiotics (secondary infection)
- antivirals
- Immunosuppressive therapies (methotrexate, azathioprine, ciclosporin)
- Biological therapies (dupilumab, tralokinumab, lebrikizumab, nemolizumab)
- Oral small molecules (baricitinib, upadacitinib, abrocitanib) for moderate/severe atopic dermatitis.
- Additional:
- Cold compresses and wet dressings
- Diet: breastfeed as long as possible, consider elimination diet
Contact dermatitis
- caused by allergens that provoke an allergic skin reaction (where most other peole can handle the chemicals without undue effect.)
- causes:
- nickel (jewellery, jeans, keys, coins)
- fragrances
- plants, dyes, chemicals, latex etc
- features:
- dermatitis isolated to site affected but can spread through contact of fingers
- dx: if in doubt refer to dermatologist for patch testing
- mx:
- key is avoiding contact so much know allergen!
- Avoid soap (only wash with water) + topical corticosteroid
- if severe short course of oral pred (starting 25-50mg for adult for 1-2 wks then reduce over 1-2wks) +/- oral abx for 2° infection
Nummular/discoid eczema
scattered, well-defined, coin-shaped and coin-sized plaques of eczema. Discoid eczema is also called nummular dermatitis
The eruption can be precipitated by:
- A localised injury such as scratch, insect bite or thermal burn
- Impetigo or wound infection
- Contact dermatitis
- Dry skin
- Varicose veins (varicose eczema)


Differentials : annular skin eruptions including
- tinea corporis
- plaque psoriasis


Management
- Protect the skin from injury.= irritated by friction, detergents, solvents, other chemicals, or excessive water.
- soap substitutes and moisturising cream
- Avoid allergens
- Topical steroids – twice daily for 2–4 weeks
- Antibiotics
- Oral antihistamines
- Ultraviolet radiation (UV) treatment

Atopic dermatitis
– criteria for dx
- Itch
- Typical morphology
- distribution (changes; baby = cheeks, face, folds of neck, scalp + extensor surfaces 🡪 child flexures of limb + groin 🡪 adult groin, ext hand, feet, neck)
- Dry skin
- Hx of atopy (or family hx -allergic rhinitis, asthma, eczema, skin sensitivities & urticarial)
- Chronic relapsing dermatitis
triggers
- dust mite (common), extremes tempt, sweating, sand pits, soap/frequent washing, pools, infection, stress, irritants (clothing, detergents), foods, scratching/rubbing, perfumes
prognosis
- most children ‘grow out of it’ as the function of their oil & sweat glands matures. Lichenification can occur w chronic atopic dermatitis.
- 60% normal skin at 6 yrs
- 90% normal skin by puberty
treatment =
- General advise = avoid soap + perfumed products (use low ph ie: dermaveen, hamiltons, qv, cetaphil) & apply emollient (sorbolene w 10% glycerol, paraffin creams – dermeze, qv moisturizing cream) immediately after bathing. Older children should have short, tepid showers. Avoid overheating/changes in t°. Wear loose clothing preferably cotton
- Consider dust mite strategies
- dust mite covers (premium grade) for bedding; wash linen in hot water >55°, consider replacing fabric on chairs + carpet
- Anti histamines
- can be given at night for itch, if used the sedating type is recommended.
- Ie: promethazine (phenergen) safe if >12yrs, can be used for short term use in children younger
- Antibiotics
- pt’s at risk of 2° infection with staph, try to prevent with anti-septic wash
- White king bleach (4%) to cool bath water at 12mls per 10l, wash scalp+face
- Topical = mupirocin 2% (bactroban) or systemic = flucloxacillin or cephalexin
- Anti-virals
- oral acyclovir as risk hsv 🡪 vesicles & ‘punched out lesions’ & pain
- Steroids =
- Face & flexures = 1% hydrocortisone (sigmacort or dermaid) once or twice daily until dermatitis settles then back to emollients. If not effective 🡪 methylprednisolone 0.1% (advantan) once daily until dermatitis settles, usually 7 days
- Alternative for face is a calcineurin inhibitor (ie: pimecrolimus = elidel)
- Treatment elsewhere on = moderately potent corticosteroid once to twice daily until settled, usually 7 – 14 days
- Betamethasone valerate 0.02% (celestone) or 0.05% (betnovate ½)
- Methlyprednisolone (advantan)
- Triamcinolone (aristocort)
- For lichen simplex or thick skin (palm or sole of foot) = potent or very potent corticosteroid once daily until settles, can take up to 3 weeks
- Betamethasone diproprionate (diprosone)
- Betamethasone valerate 0.1% (betnovate)
- Mometasone 0.1% (elocon)
- Face & flexures = 1% hydrocortisone (sigmacort or dermaid) once or twice daily until dermatitis settles then back to emollients. If not effective 🡪 methylprednisolone 0.1% (advantan) once daily until dermatitis settles, usually 7 days
- Nb: if severe dermatitis may need occlusive dressings +/- hosp admission. Apply moisturizer and/or corticosteroid then apply wet dressing followed by dry. Left on overnight or changed 4x during day. Inappropriate use leads to folliculitis, infection, maceration or excessive dryness. A wet compress can be applied to affected area for 5-10mins to relieve itch, moisturize after.
- advise on steroids
- use cream base if weeping, use ointment base if dry or lichenification & lotion based if hairy areas
- use steroid for 7-14d & ask to return for review if doesn’t settle in expected timeframe
- if flares can have short term use 7-14days then switch to emollient
- if moderate or more potent steroid one daily administration is usually enough
- staph eradication
- quarter fill bath w water + add 45ml (3 tbls) of household bleach (ie: white king.
- Soak in bath for 5 minutes but don’t immerse face
- Rinse skin in fresh water & pat dry using old towels to avoid bleaching coloured towels.
- Immediately apply prescribed creams + moisturizer. Repeat twice a week or as suggested by your doctor.
Ichthyosis vulgaris

excessive dry, scaly skin
It is the most common form of the inherited ichthyoses
- Treatments
- Keep skin hydrated
- Apply emollients with high lipid content, such as lanolin cream (a sebum-like substance derived from wool-bearing animals).
- Keep skin hydrated
- Treatments to reduce scale
- Bathe in salt water.
- Apply creams or lotions containing salicylic acid, glycolic acid, lactic acid or urea to exfoliate and moisturise skin. These may irritate active eczema.
- Oral retinoids such as acitretin or isotretinoin can be prescribed in severe cases.
Pityriasis alba

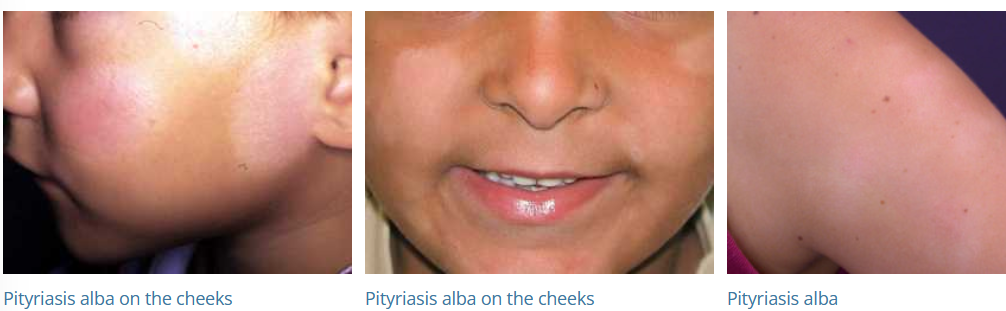
- Pityriasis alba is a low-grade type of eczema/dermatitis mainly seen in children 3-16 years.
- form of subacute atopic dermatitis
- very common mild condition, worse in summer (b/c won’t tan) & dark skinned children
- self limiting and will clear up in months, sometimes years
- diagnosis
- rule out other causes of pigmentation
- Wood lamp examination: the hypopigmentation of pityriasis alba does not enhance, and there is no fluorescence
- Scrapings for mycology: microscopy and fungal culture are negative in pityriasis alba
- Skin biopsy: biopsy is rarely required, but may reveal mildly spongiotic dermatitis and reduction in melanin.
- rule out other causes of pigmentation
- mx: non-soap cleanser, emollients. Hydrocortisone rarely needed or pimecrolimus
Treatment
No treatment is necessary for asymptomatic pityriasis alba.
- A moisturising cream may improve the dry appearance.
- A mild topical steroid (0.5-1% hydrocortisone) may reduce redness and itch if present.
- Calcineurin inhibitors (pimecrolimus cream and tacrolimus ointment) may be as effective as hydrocortisone and have been reported to speed recovery of skin colour.
Asteatotic dermatitis


A “Cracked Porcelain” Appearance
Caused by water loss from the stratum corneum.
This occurs because of a breakdown of the skin barrier due to genetic predisposition and injury by environmental factors. These include:
- Low humidity (winter, desert, high altitude, travel, use of dehumidifier or fan heater)
- Excessive bathing especially using soaps and detergents
Who gets asteatotic eczema? – Asteatotic eczema can occur in anyone with very dry skin.
- It most often affects older people.
- It is also a complication of inherited and acquired forms of ichthyosis.
- Systemic causes include underactive thyroid (myxoedema), malnutrition (zinc and fatty acid deficiencies), severe weight loss and lymphoma.
- Drugs can cause asteatotic eczema, particularly retinoids (acitretin, isotretinoin), diuretics and protein kinase inhibitors.
treatment.
- Consider factors that have caused dry skin: bathe less frequently, use a cream cleanser instead of soap, do not expose skin to direct heat.
- Apply thick emollients and moisturisers such as petroleum jelly/petrolatum or oily cream several times daily — after a few days, thinner ones such as non-ionic cream should be adequate.
- Apply mild topical steroid cream or ointment to reddened skin for a few days; hydrocortisone cream or ointment is often sufficient.
- A more potent topical steroid may be necessary if the eczema is severe.