Scabies
- Scabies is a highly infectious skin infestation caused by a tiny mite called Sarcoptes scabiei (
- common in
- school-aged children
- closed communities (nursing homes and in some Indigenous communities)
- Pathology
- The female mite burrows just beneath the skin in order to lay her eggs.
- She then dies.
- The eggs hatch into tiny mites that spread out over the skin and live for only about 30 days.
- mite antigen, in its excreta, causes a h ypersensitivity rash.


| Differential diagnoses of classical scabies | |||
| Insect bites | Infections | Dermatitis | Immune-mediated |
| Mosquitos | Folliculitis | Eczema | Papular urticarial |
| Midges | Impetigo | Contact dermatitis | Bullous pemphigoid |
| Fleas | Tinea | Pityriasis rosea | |
| Bedbugs | Viral exanthems | ||
Diagnosis:
- Based on typical appearance and distribution of lesions/rash, and presence of burrows.
- Classic burrow: linear intra-epidermal tunnel (short wavy greyish/white threadlike elevations, 2-10 mm).

- Confirm diagnosis by identifying mite, eggs, or faecal matter through:
- Removing mite with needle tip from burrow.
- Skin scraping and microscopic examination with KOH.
- Dermatoscope identification.
Differential Diagnoses:
| Insect bites | Infections | Dermatitis | Immune-mediated |
|---|---|---|---|
| Mosquitos | Folliculitis | Eczema | Papular urticarial |
| Midges | Impetigo | Contact dermatitis | Bullous pemphigoid |
| Fleas | Tinea | Pityriasis rosea | |
| Bedbugs | Viral exanthems |
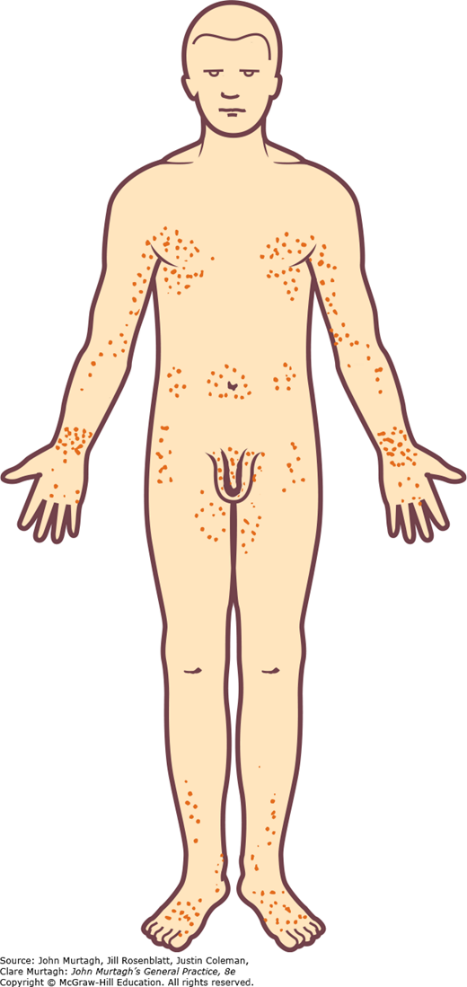
CLINICAL FEATURES
- Intense itching (worse with warmth and at night)
- Erythematous papular rash
- Usually on hands and wrists
- Common on male genitalia
- Also occurs on elbows, axillae, feet and ankles, nipples of females
- Genital scabies causing severe pruritus, showing bruising on the upper thighs from intense scratching
- Typical distribution of the scabies rash
SPREAD
- The mites are spread from person to person through close personal contact (skin to skin), including sexual contact.
- spread through contact with infested clothes or bedding, although this is uncommon.
- Sometimes the whole family can get scabies.
- The spread is more likely with overcrowding and sexual activity.
TREATMENT
| Treatment of typical scabies | ||||||
| Age | Medication | Brand names | Route | Dose and administration | Frequency | |
| First-line treatment | ||||||
| Younger than 2 months of age | Crotamiton | Eurax | Topical | Apply to whole body, wash off after 24 hours | Repeat daily for three days | |
| Older than 2 months of age | Permethrin 5% | Lyclear | Topical | Apply to whole body, wash off after eight hours | Can repeat after 7–14 days if ongoing symptoms | |
| Second-line treatment | ||||||
| Older than 6 months of age | Benzyl benzoate 25% | AscabiolBenzemul | Topical | Dilute to 6.25% for infants 6 months to 2 years of age Dilute to 12.5% for children 2–12 years of ageApply to whole body, wash off after 24 hours | Repeat once after 7–14 days | |
| Third-line treatment | ||||||
| 5 years of age or older | Ivermectin | Stromectol | Oral | 200 μg/kg Contraindicated if <15 kg, pregnant, or breastfeeding | Repeat once after 7–14 days | |
- Permethrin
- best applied to clean, cool, dry skin
- Apply to entire body from jawline down (including under nails [with a nail brush], in flexures and genitals).
- washed off after eight hours.
- All household contacts should be treated at the same time.
- If the first application is thorough, then no repeat dose is required, as permethrin is active against all stages of the parasite’s life cycle.
- If symptoms persist, a repeat application 7–14 days after the first treatment.
- Permethrin is highly effective and generally well tolerated, but success may be hindered by
- non-adherence of asymptomatic contacts
- inadequate application
- incidental washing off of the therapy.
- Benzyl benzoate 25%
- is the second-line topical agent.
- commonly causes skin irritation, and should be diluted with water for children and infants
- It is applied and then left for 24 hours before being washed off.
- Ivermectin
- macrocyclic lactone antiparasitic derived from fermentation products of the bacterium Streptomyces avermitilis.
- has very broad antiparasitic activity
- onchocerciasis (river blindness)
- lymphatic filariasis
- soil-transmitted helminths.
- active against the scabies mite, but not its eggs, and has a short half-life of 12–56 hours.
- Therefore, repeat dosing 7–14 days after the first dose is required to kill newly hatched mites.
- Ivermectin is the only currently available oral agent that is effective against scabies.
- advantage of ivermectin is its oral formulation, increasing the likelihood that household contacts will adhere to treatment.
- Adverse effects
- itch, headache, dizziness, and abdominal and joint pain
- does not cross the blood–brain barrier in humans.
- not recommended for use in
- children younger than 5 years of age or weighing less than 15 kg.
- pregnant and breastfeeding women

- General Measures
- Treat the whole family at the same time even if they do not have the itch.
- Decontaminate bedding, clothing, and towels used in the previous 4 days:
- Wash at 60°C and dry in a hot dryer, dry-clean, or seal in a plastic bag for 72 hours.
- Shoes/non-washable items: Seal in plastic bag for at least 3 days.
- Mites do not survive more than 72 hours away from human skin.
- Environmental measures for scabies infection
- role of transmission of scabies other than person-to-person transmission is controversial
- Scabies mites are highly susceptible to dehydration away from the human host, surviving for only three days.
- transmission from fomites is uncommon
- therefore environmental cleaning(hot water laundry washes etc..) for classical scabies is unnecessary, aside from institutional settings
Treatment of associated impetigo
- secondary bacterial infection
- initial treatment with antibiotics and removal of crusts
- followed by topical scabies treatment
- Flucloxacillin in adults and cephalexin in children (more palatable than flucloxacillin) are the preferred choice of antibiotics in non-remote settings where S. aureus is the most likely pathogen
- In remote settings, S. pyogenes is the primary driver of infection, and additional treatment options include short-course trimethoprim-sulfamethoxazole or intramuscular benzathine penicillin
CRUSTED (NORWEGIAN) SCABIES

- Rare
- majority of cases have a relatively small number of mites (as few as 15), infestation with thousands or millions will cause the condition of crusted scabies.
- places patients at high risk for invasive bacterial infection, sepsis and mortality
- Diagnosis is made on a scraping which reveals vast numbers of lesions.
Treatment usually requires hospital admission for isolation and intensive treatment with a combination of topical scabicides, oral ivermectin and topical keratolytics.
- Public health considerations
- Because of the prolonged asymptomatic phase, scabies is often spread from person-to-person before a diagnosis is made
- scabies outbreak is indicative of transmission within the institution for at least several weeks.
- Widespread outbreaks may occur in closed communities, such as hospitals, RACFs and prisons, or areas where overcrowding is common.
- patient should be isolated in a single room until 24 hours after the first treatment has been completed, if possible, and staff and visitors should use contact precautions during this period.
- The index case should be treated, along with staff or visitors who had direct contact with them.