Tinea cruris
- jock itch/tinea cruris is a common infection of the groin area in young men
- caused by Trichophyton rubrum
- The dermatophytes responsible for tinea thrive in damp, warm, dark sites.
- It is transmitted by towels and other objects, particularly in locker rooms, saunas and communal showers
- Differentials
- Simple intertrigo
- Skin disorders:
- psoriasis
- seborrhoeic dermatitis
- dermatitis/eczema
- Fungal:
- Candida
- tinea
- Erythrasma
- contact dermatitis

- CLINICAL FEATURES
- Itchy rash
- More common in young males
- Strong association with tinea pedis (athlete’s foot)
- Usually acute onset
- More common in hot months—a summer disease
- More common in physically active people
- Related to chafing in groin (e.g. tight pants, and especially synthetic jock straps)
- Scaling, especially at margin
- Well-defined border
- The feet should be inspected for evidence of tinea pedis.
- If left untreated, the rash may spread, especially to the inner upper thighs, while the scrotum is usually spared.
- Spread to the buttocks indicates T. rubrum infection.
- Complications:
- Maceration and secondary infection with bacteria or candida
- Secondary excoriation, lichenification, and pigmentation
- Tinea incognita due to use of topical steroids
- DIAGNOSTIC AIDS
- Skin scrapings should be taken from the scaly area for preparation for microscopy
- Wood’s light may help the diagnosis, particularly if erythrasma is suspected.
- MANAGEMENT
- Fastidious drying of skinfolds.
- Apply topical terbinafine 1% cream or gel once or twice daily for 7–14 days or an imidazole topical preparation (e.g. miconazole or clotrimazole cream).
- Apply tolnaftate dusting powder bd when almost healed to prevent recurrence.
- If itch is severe, a mild topical hydrocortisone preparation (additional) can be used.
- For persistent or recurrent eruption, use oral terbinafine for 2–4 weeks or griseofulvin for 6–8 weeks.
- Candida intertrigo
- Candida albicans superinfects a simple intertrigo and tends to affect patients with predisposing factors (e.g. broad-spectrum antibiotic therapy, diabetes, general debility, immune incompetence, obesity, immobility).
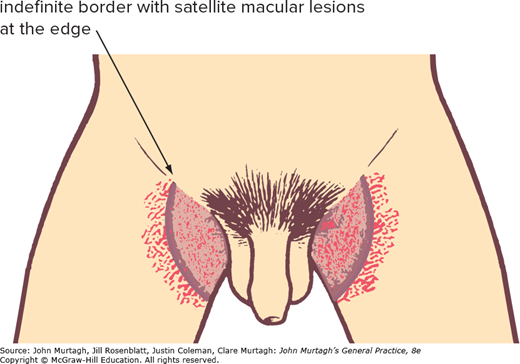
- CLINICAL FEATURES
- Erythematous, macerated rash
- Occurs in flexures, submammary area and other skinfolds
- Less well-defined margin than tinea
- Associated satellite lesions and whitish discharge
- Yeast may be seen on microscopy
TREATMENT
- Treat predisposing factors where possible.
- Apply an imidazole preparation such as miconazole 2% or clotrimazole 1%, twice daily for 2 weeks.
- Use short-term hydrocortisone cream for itch or inflammation (long-term aggravates the problem).