SIADH
Syndrome of inappropriate antidiuretic hormone secretion (SIADH) Summary:
- can occur secondary to medications, malignancy, pulmonary disease, or any disorder involving the central nervous system.
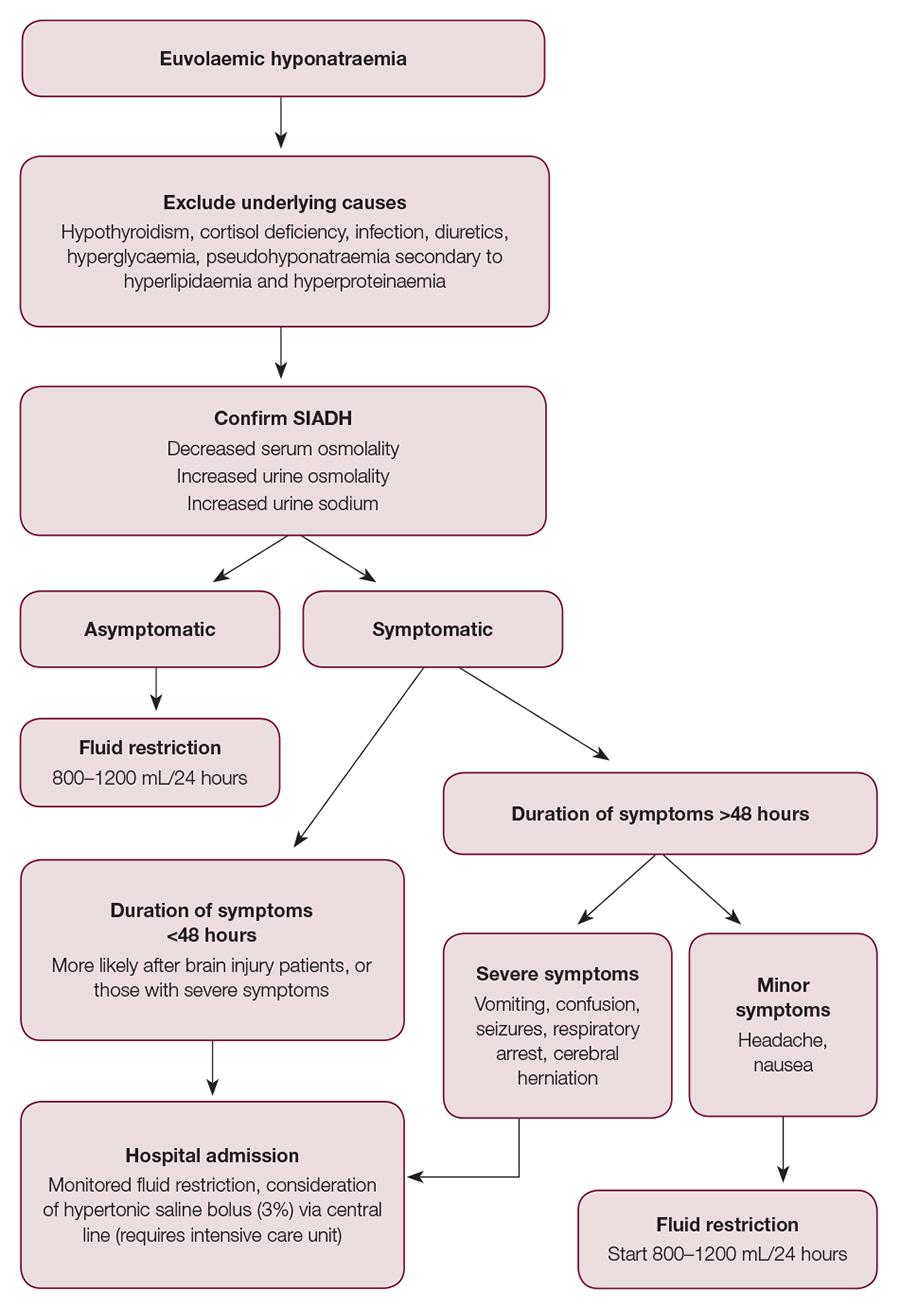
- Diagnosis is made on the basis of clinical euvolaemic state with low serum sodium and osmolality, raised urine sodium and osmolality, and exclusion of pseudohyponatraemia and diuretic use.
- Fluid restriction of 800–1200 mL/24 hours is the mainstay of treatment
- Patients with severe hyponatraemia and symptoms of altered mental state or seizures should be admitted to hospital for monitoring of fluid restriction and consideration of hypertonic saline. A rapid increase in sodium levels can precipitate osmotic demyelination and, as such, the increase in serum sodium should not exceed 10 mmol/L in 24 hours or 18 mmol/L in 48 hour
Pathology
- In SIADH, hyponatraemia is due to inappropriate secretion of antidiuretic hormone (ADH).
- In a normal physiological state, ADH is released in response to increased serum osmolality, whereas in SIADH, ADH secretion is unregulated.
- Increased production/ectopic production or increased sensitivity to ADH results
🡪 in increased water permeability of the renal distal tubule and collecting duct through aquaporin insertion.
- The subsequent dilutional hyponatraemia activates volume-sensitive natriuretic mechanisms, causing salt excretion and maintaining euvolaemic hyponatraemia
Underlying causes of SIADH
- Neurosurgical or neurological – increased ADH release:
- Guillain-Barré syndrome
- Subarachnoid haemorrhage
- Subdural haemorrhage
- Infective – increased ADH release:
- Meningitis
- Encephalitis
- Abscesses
- Human immunodeficiency virus
- Sarcoidosis
- Respiratory – increased ADH release:
- Tuberculosis
- Pneumonia
- Pneumothorax
- Atelectasis
- Asthma
- Medications – increased ADH release:
- Antidepressants (eg sertraline)
- Anticonvulsants (eg carbamazepine, leveteiracetam)
- Antipsychotics (eg haloperidol)
- Anti-inflammatory drugs
- Ecstasy
- Cyclophosphomide
- Malignancy – ectopic ADH production:
- Nasopharyngeal
- Mesothelioma
- Pancreatic
- Gastrointestinal
- Lymphoma
- Sarcoma
Diagnosis of SIADH
- decreased serum osmolality (<275 mOsm/kg)
- increased urine osmolality (>100 mOsm/kg)
- euvolaemia
- increased urine sodium (>20 mmol/L)
- no other cause for hyponatraemia (no diuretic use and no suspicion of hypothyroidism, cortisol deficiency, marked hyperproteinaemia, hyperlipidaemia or hyperglycaemia).
Investigations for underlying causes
- biochemistry looking at serum sodium level
- serum osmolality
- urine osmolality (random sample collected at same time as serum sample)
- thyroid function tests
- morning cortisol level if hyponatraemia is potentially related to Addison’s disease
- computed tomography (CT) of the head if a neurosurgical condition is suspected (eg subarachnoid haemorrhage, subdural haematoma)8
- chest X-ray if pulmonary causes of SIADH are suspected.
MaNAGEMENT