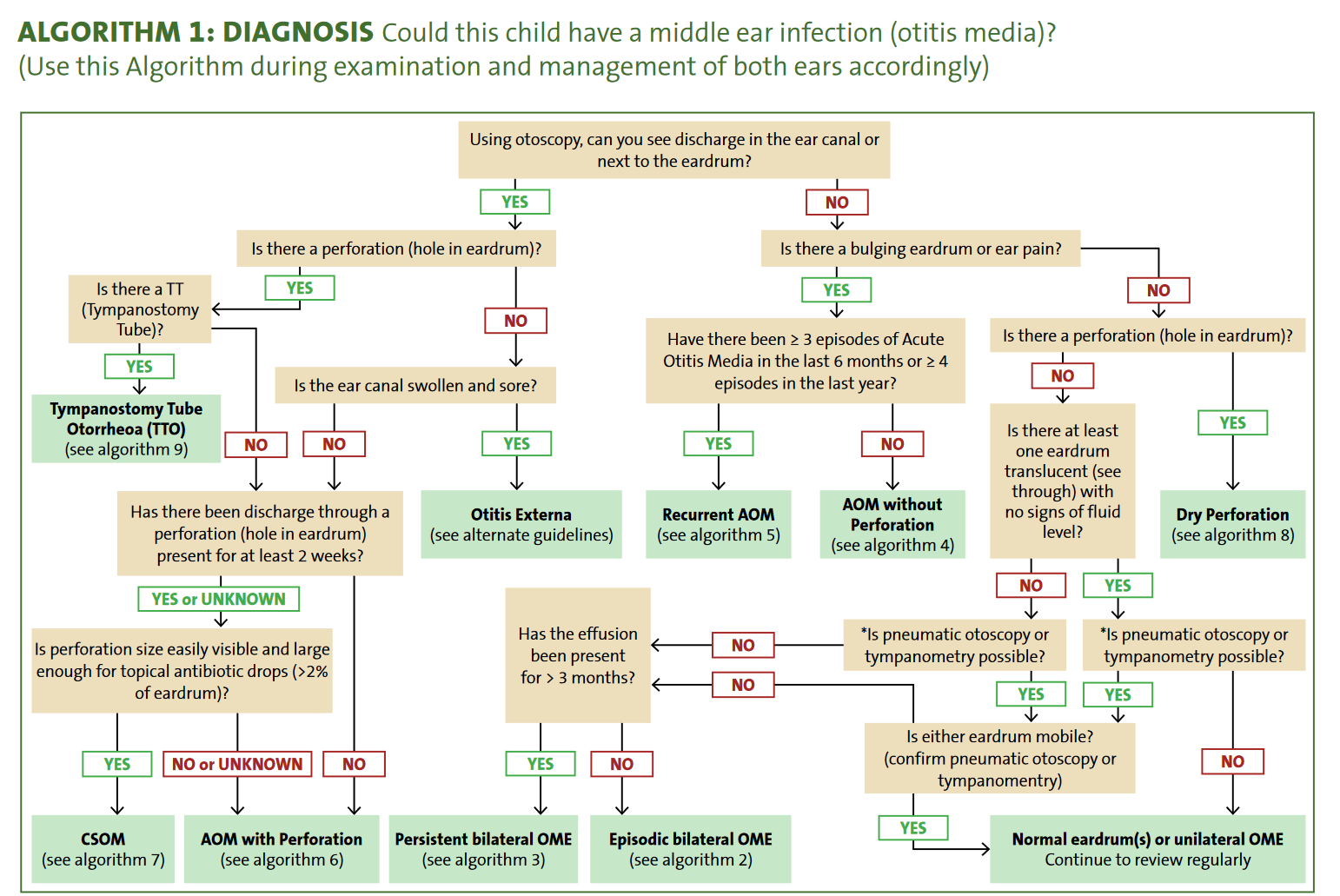
Acute Otitis Media
Otitis Media Terms:
| Otitis Media (OM): | Refers to all forms of inflammation and infection of the middle ear.Active inflammation or infection is nearly alwaysassociated with a middle ear effusion (fluid in themiddle ear space). |
| Acute Otitis Media (AOM): | General term for both acute otitis media with and without perforation. It is defined as the presence of fluid behind the tympanic membrane plus at least one of the following: – bulging tympanic membrane – red tympanic membrane -recent discharge of pus – fever – ear pain – irritability A bulging tympanic membrane, recent discharge of pus, and ear pain are the most reliable indicators of AOM. |
| Acute Otitis Media without Perforation(AOMwoP) | The presence of fluid behind the tympanic membrane plus at least one of the following: – bulging tympanic membrane – red tympanic membrane – fever – ear pain – irritability A bulging tympanic membrane and/or ear pain are the most reliable indicators of AOMwoP. |
| Acute Otitis Media with Perforation (AOMwiP): | Discharge of pus through a perforation (hole) in the tympanic membrane within the last 2 weeks. The perforation is usually very small (a pinhole) when the tympanic membrane first ruptures. The perforation can heal and re-perforate after the initial onset of AOMwiP. The size of the perforation should be recorded, as this directs management, and duration of discharge is often difficult to establish. |
| Otitis Media with Effusion (OME): | Presence of fluid behind the tympanic membrane without any acute symptoms. Other terms have also been used to describe OME (including ‘glue ear’, ‘serous otitis media’ and ‘secretory otitis media’). OME may be episodic or persistent. A type B tympanogram or reduced mobility of the tympanic membrane on pneumatic otoscopy are the most reliable indicators of OME. |
| Recurrent Acute Otitis Media (rAOM): | occurrence of 3 or more episodes of AOM in a 6-month period, or occurrence of 4 or more episodes in the last 12 months |
| Episodic OME: | OM as defined above of duration less than three months. |
| Persistent (Chronic) Otitis Media with Effusion(pOME): | Presence of fluid in the middle ear for more than 3 months without any acute symptoms or signs of inflammation. |
| Chronic Suppurative Otitis Media (CSOM): | Persistent ear discharge through a perforation in the tympanic membrane lasting 2 weeks or more and Tympanic membrane perforation large enough to allow penetration of topical antibiotics into the middle ear space (generally > 2% of the pars tensa). The size of the perforation should be determined and recorded, as this directs management, and duration of discharge is often difficult to establish. |
Dry Perforation (DP): | Presence of a perforation in the tympanic membrane without any signs of discharge or fluid behind the tympanic membrane. Some people also refer to this as inactive CSOM. |
Cholesteotoma: | Abnormal growth of skin cells in the middle ear, which continues to grow eventually causing erosion of surrounding structures (middle ear ossicles, facial nerve, base of skull), resulting in hearing loss, facial paralysis or intracranial complications |

| AOM | OME |
|---|---|
| Tympanic membrane is typically: – bulging red white or pale yellow | Tympanic membrane is typically: – retracted or in the neutral position – amber or blue – A fluid level or bubbles may be seen behind the tympanic membrane |
- Usually viral, can be bacterial or combined
- Regardless usually self limiting
- Spontaneous resolution 80% of children in 2-3 days. Symptoms may be up to 8 days
- Bacterial – strep pneumonia, Hemophilus influenzae, Moraxella Catarrhalis
- Do not accept otitis media as the sole diagnosis in a sick febrile young child without exclusion of more serious causes (see Febrile child)
- Diagnosis requires
- Acute onset
- Signs of middle ear inflammation + middle ear effusion
- Avoid the routine use of antibiotic treatment for acute otitis media
- considered for immediate Abx if Redflags (<6 months, Cochlear implant, Immunocompromised, ATSI, Possible suppurative complication_
Examination
- Systemically unwell
- Ear examination:
- Signs of acute inflammation of the tympanic membrane (TM): bulging, red, opaque TM
- a red TM alone is not AOM.
- The most common cause is a viral upper respiratory tract infection (URTI)
Diagnosis
- Middle ear inflammation AND middle ear effusion
- Acute onset of either
- Bulging of tympanic membrane
- Ear discharge/Otorrhoea (perforation + effusion) – provided not otitis externa
- In Infants, especially <6 months old
- the diagnosis of AOM and OME can be inaccurate
- Other diagnoses should be fully considered (see Febrile child)
- If cannot visualize – ensure follow up, or review ENT/audiologist
- Middle ear effusion – immobile tympanic membrane on pneumatic otoscopy or a type B tympanogram (usually regular otoscopy can’t tell)
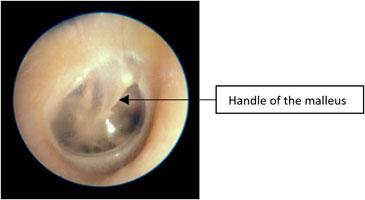 |  |  |
| Normal Tympanic Membrane TM is translucent The handle of the malleus is vertical No erythema | Injected Tympanic Membrane Pink/red TM Often seen with fever, eustachian tube obstruction or viral URTITM is transparent (there is no middle ear effusion)The handle of the malleus is well seen and is more horizontal | Bulging and red tympanic membrane in AOM Loss of the TM landmarks, especially the handle of the malleusTM is opaque, may be red from inflammation or white from pus in the middle ear |
 |  |  |
| Otitis Media with Effusion (OME) “glue ear” TM is retracted with prominence of the handle of the malleus, which is also drawn in/more horizontal TM may be bulging or have an air-fluid level behind the TM Yellow/amber appearance is consistent with fluidLight reflex on otoscopic examination | Perforated Tympanic Membrane with otorrhoea | Otitis Externa Ear is tender to examine Skin of the external ear canal is swollen and there can be thin pus |
Treatment

- Regular analgesia
- Panadol/Neurofen
- Topical analgesia = Lignocaine aqueous 2% 3 drops intraaurally 2hrly PRN

- Give Abx if
- Infants < 6 months
- 2 bilateral infection
- Systemically unwell – lethargic, pale, irritable (not just fever)
- Otorrhea/perforation
- High risk ATSI
- High risk complications e.g. Immunocompromised
- Craniofacial abnormalities
Antibiotics
- No Abx for 48hrs of SSx if no improvement
- Amoxicillin 30mg/kg/dose BD for 5 days
- Azithromycin 10-20 mg/kg/day single dose orally ~3 days recommended in eTGA for
- neonatal conjunctivitis
- pertussis
- mild pneumonia
- i.e. OK for < 6 mo) where adherence to antibiotics is likely to be poor or whose families do not have refrigeration
- If no improvement
- Alternative diagnosis
- Switch to Amoxicillin-Clavulanate 22.5mg/kg/dose BD
Also is recommended first line if
- a child has received amoxicillin in the last 30 days
- has concurrent purulent conjunctivitis
- has a history of recurrent acute otitis media unresponsive to amoxicillin
- Doses up to 45 mg/kg (max 1 g) bd can be used in those at high risk of penicillin resistant pneumococci such as ATSI children or in recurrent AOM
- For chronic otorrhoea
- consider addition of topical ciprofloxacin 0.3% drops 12hours until free of discharge for at least 3 days
- For children with penicillin hypersensitivity:
- Delayed:
- Cefuroxime (3 months to 2 years: 10 mg/kg max 125 mg
- 2 years or older : 15 mg/kg max 500 mg) orally, bd for 5 days
- Immediate:
- Trimethoprim+sulfamethoxazole (child 1 month or older)
- 4+20 mg/kg
- max 160+800 mg orally, bd for 5 days
- Trimethoprim+sulfamethoxazole (child 1 month or older)
- Delayed:
Recurrent OM

- = 3 or more in 6 months, or 4 in 12 months
- Risk factors
- child care
- allergic rhinitis
- adenoid disease
- structural abnormalities e.g. Cleft palate, Downs
- exposure to smoke
- SES disadvantage e,g, crowding
- High risk indigenous includes
- lives in remote communities
- less than 2 years of age
- has had their first episode of OM before 6 months of age
- with a family history of CSOM
- with a current or previous TM perforation
- with craniofacial abnormalities
- cleft palate, Down Syndrome
- immunodeficiency
- cochlear implants
- developmental delay
- with hearing loss
- with severe visual impairment.
- Ensure S. Pneumoniae vaccination up to date
- Consider referral – ?myringotomy + grommets
- Tympanic membrane perforation with AOM common – shouldn’t alter AOM management
- Rare complications – mastoiditis, facial palsy
Complications
- Facial nerve palsy
- Unilateral facial droop / lower motor neurone signs
- Intracranial complications
- (including meningitis, brain abscess and subdural empyema)
- AOM with fever, headache, vomiting, irritability, or altered conscious state, with or without focal neurologic signs
- Sepsis
- Toxic features
- Hearing Loss: Temporary or permanent hearing loss can occur due to fluid build-up or damage to the structures of the middle ear.
- Speech or Developmental Delays: In children, recurrent OM can lead to delays in speech and language development due to hearing loss.
- Tympanic Membrane Perforation: Repeated infections can weaken and eventually lead to perforation of the eardrum.
- Cholesteatoma: An abnormal skin growth in the middle ear behind the eardrum can develop following recurrent infections.
- Scarring of the Tympanic Membrane: Repeated episodes can lead to scarring, which may affect hearing.
- Acute Mastoiditis (AM)
- Acute mastoiditis, although rare, is the most common suppurative complication of AOM and may be associated with intracranial complications
- diagnosis of AM is based on post auricular inflammatory signs (erythema, oedema, tenderness or fluctuance), a protruding auricle often with external auditory canal oedema and signs of AOM (see image below)
- Requires prompt treatment with appropriate intravenous antibiotics (eg flucloxacillin plus 3rd generation cephalosporin)
- spread of infection are rare
- Facial nerve palsy secondary to AOM should be discussed with ENT
