Dental
Gingivitis

- red, swollen gingivae adjacent to teeth with halitosis
- bleeds with gentle probing
- not painful (unless assoc with primary HSV infection)
- secondary to poor dental hygiene
- treatment: chlorhex mouth wash BD, abx if any abscess formation

Dry socket
- A dull throbbing pain develops two to four days after a mandibular tooth extraction.
- It rarely occurs in the maxilla.
- Smoking is a major predisposing factor as it reduces the blood supply.
- The tissue around the socket is very tender and white necrotic bone is exposed in the socket.
- Halitosis is very common.
- Treatment
- The area should be irrigated thoroughly with warm saline solution.
- If loose bone is present, local anaesthesia may be necessary to allow thorough cleaning of the socket.
- Patients should be shown how to irrigate the area and told to do this regularly.
- Analgesics are indicated, but pain may persist for several days.
- Although opinion is divided as to whether or not dry socket is an infective condition, do not recommend the use of antibiotics in its management

Trauma
- Management depends if primary or permanent teeth impacted
- Primary teeth are never re-positioned, splinted or replaned
- But do need to treat to prevent risks to developing permanent teeth
- Avulsion of a permanent tooth is a dental emergency
- Check tetanus immunisation
- Assessment
- Symmetry
- Gingival/mucosal injury
- Type of tooth
- Type of dental injury
- Bite occlusion
- Healing – swab with chlorhexidine for 14 days, soft diet
Loose or displaced teeth (periodontal displacement injuries)
| Injury | Examination findings | Management |
| Concussion = An injury to tooth-supporting structures without abnormalloosening or displacement but with marked reaction to percussion. | Tender but firm | Review by community dentist Usually heal without intervention |
| Subluxation = Slight increase in mobility but without clinically or radiographically demonstrable displacement of the tooth | Tender loose tooth, blood around gum | Refer to hospital dental registrar if very loose* Swab or rinse with 0.12% chlorhexidine twice a day for 10–14 days |
| Lateral luxation Extrusion Intrusion | Anteriorly or posteriorly displaced Partially out of socket Pushed into socket | repositioning and splintingPrimary: monitored or extracted Permanent: usually repositioned or splinted under local or general anaesthetic spontaneous eruption or orthodontic extrusion. |
| Avulsion | Complete displacement from socketNote: need to differentiate avulsion from fully intruded tooth (may need x-ray) | Primary: not reinserted Permanent: place in milk or saline while awaiting assessment (do not use water or scrub tooth), do not handle tooth root, if possible return to socket and bite down with gauze to hold tooth in position, support tooth with alfoil wrap, best prognosis if “dry-time” less than 60 minutes |
Fractured teeth
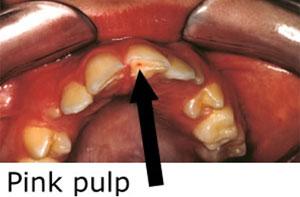
- Enamel is white, dentine is yellow, pulp is pink
| Injury | Examination findings | Management |
| Primary | Enamel or dentine only | See community dentist within a few weeks |
| Primary | Exposed pulp (pink and painful) | Refer to hospital dental registrar for likely extraction |
| Permanent | Enamel or dentine only | See community dentist within a few weeks |
| Permanent | Exposed pulp (pink and painful) | Refer to hospital dental registrar Keep tooth or fragments in milk for possible rebonding |
 |  |
Injuries to the supporting bone
- Check that the child’s bite is normal
- Get an OPG and other views as required
- Refer to both dental and maxillofacial (obvious jaw fractures)
- Dental and maxillofacial follow-up is recommended for all patients with mandibular or maxillary fractures, even when undisplaced
Injuries to the gingivae or oral mucosa
- Oral mucosa degloving injuries (gingivae stripped from underlying bone) can be missed if the lips are not firmly lifted away from the gum as part of the examination
- The chin is often swollen and tender in mandibular degloving injuries
- Degloving injuries and deep lacerations or tears require operative cleaning, debridement and suturing to reduce the risk of osteomyelitis
- Refer to hospital dental registrar
- Manage intra and extra oral lacerations as required
Dental socket bleeding
- Can occur after treatment if child disturbs blood clot or due to a bleeding disorder
- Management:
- assess and manage haemodynamic status
- clean mouth with cold water
- provide local pressure with gauze soaked in water or saline (bite down if able for 30 minutes)
- if ongoing bleeding consider gauze soaked in tranexamic acid
- may need surgical dressing and suturing
Natal teeth
- Usually do not require intervention
- Indications for extraction: very loose, inhalation risk, difficulties breastfeeding or traumatic ulcerations of the tongue/frenulum/lip
Thumb-sucking and dummies
- Prolonged thumb-sucking and dummy use can cause problems with front teeth alignment, open bite and a “V-shaped” palat
Dental caries
- Dental caries (tooth decay) occurs in more than 40% of Australian children and can begin as soon as teeth erupt during infancy
- “Early childhood caries” mainly affects the upper front teeth, and is seen in both prolonged breast and bottle-fed children (>18 months) who continue to feed frequently at night or who comfort suck to sleep once teeth have erupted
- Infants can have their teeth and gums wiped with a clean cloth or baby toothbrush
- From 12 months twice daily brushing with a smear of paediatric fluoridated toothpaste supervised or performed by parents (for children under 8 years) and annual dental review helps prevent caries and complications
- Routine dental care should be provided in the community rather than by hospitals, except for children with chronic illness that may be impacted by dental caries (eg cancer, cardiac disease, immunodeficiency, bleeding disorders, special needs) or where general anaesthetic is required