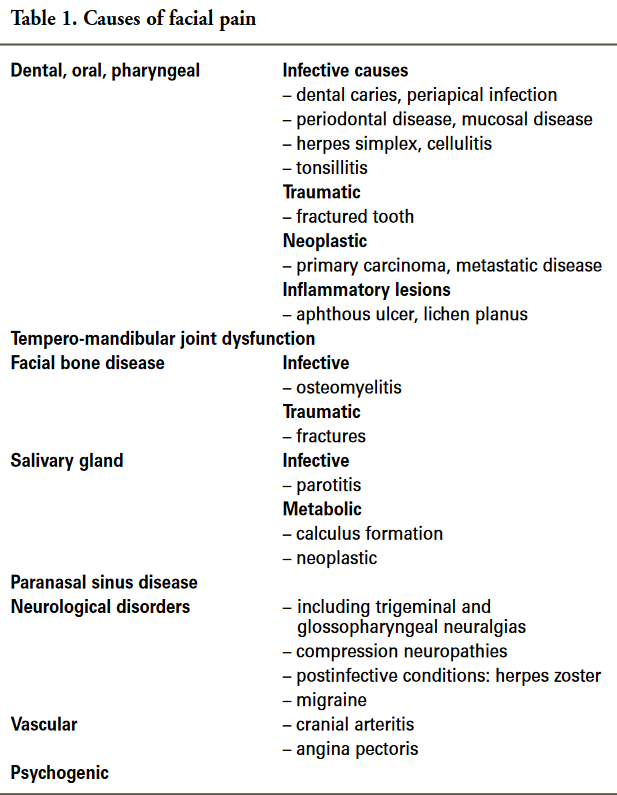
Facial pain
- In the majority of cases, facial pain is caused by dental disease or temporomandibular dysfunction.
- Usually the cause can be determined by careful history and examination.
- Atypical facial pain may require more extensive investigation with imaging and laboratory investigation as causes such as
- nasopharyngeal carcinoma
- vascular disease
- thalamic infarcts
may not be identified by clinical assessment.
- Depression or other psychogenic causes should always be considered.
- As facial pain does not cross the midline
- bilateral pain raises the possibility of a psychosomatic cause.
- Depression and anxiety are more common in elderly women living alone, although it is seen at all ages.
- Low-dose tricyclic antidepressants taken before retiring, together with a supportive environment, often lead to significant pain reduction in these patients.
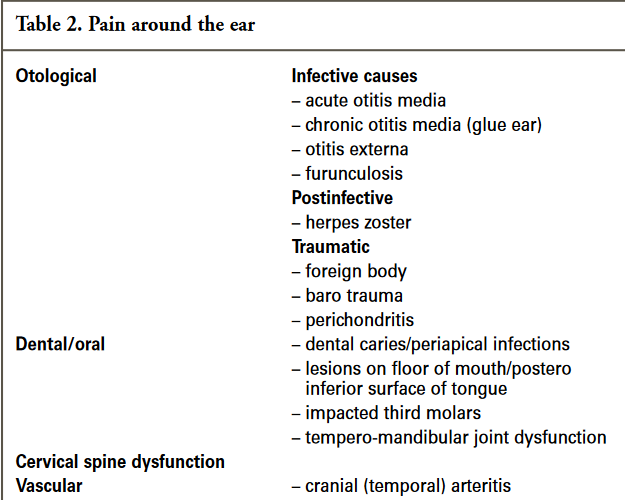
- Temporal arteritis may cause pain around the ear, eye symptoms, and pain on chewing, and is an important differential diagnosis, particularly in the elderly.
Maxillary sinusitis
- Acute
- pain in the region of the upper molar teeth, which may also be tender to percussion.
- Chronic
- from infection, allergy or airway abnormality.
- Symptoms
- nasal obstruction and discharge
- malaise and halitosis
- Pain in the malar region
- frontal headache and tenderness over the sinus and upper molar teeth
- aggravated by running and bending over
- Sinusitis can be a sequel to dental pulpitis of an upper molar if periapical infection spreads to the floor of the sinus.
Trigeminal neuralgia
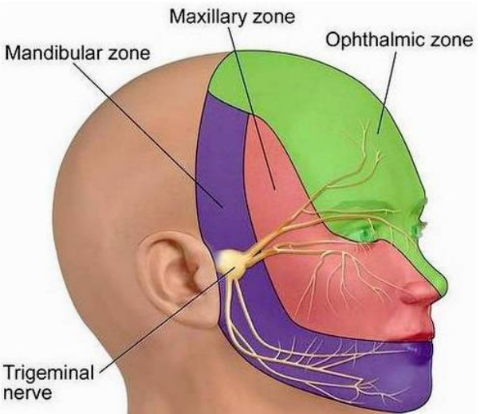
- a unilateral disorder characterised by brief electric shock-like pains, abrupt in onset and termination, limited to the distribution of one or more divisions of the trigeminal nerve
- Symptoms
- brief electric shock-like pains
- abrupt in onset and termination
- limited to the distribution of one or more divisions of the trigeminal nerve
- site
- pain is unilateral in the distribution of the trigeminal nerve
- V3- in 20% of cases
- V2,V3 – in 40% of cases
- V1,V2,V3 – in 15% of cases
- bilateral in 3% of patients and rarely is the pain active on both sides at the same time
- periodicity
- episodic and sudden onset of pain
- lasting a few seconds to minutes and stopping suddenly
- many attacks a day
- there is a refractory period between each attack
- pain might then go into remission for a few weeks or months; pain free intervals gradually shortens between episodes with time (pain often gets longer with time)
- character
- electric shock like, sharp, shooting
- severity
- very severe attacks, pain may be so severe that the patient will only be able to point to the site of the pain and not be able to touch the site
- can get milder when patients are given drug treatment
- factors affecting pain
- pain can be provoked by
- light touch to the face
- eating
- cold winds
- vibrations
- repeated stimulation may alleviate symptoms temporarily and permit pain free activity, e.g. to eat food
- pain can be provoked by
- associated factors
- Autonomic symptoms
- conjunctival injection, lacrimation, nasal congestion or rhinorrhoea, eye lid oedema, ptosis, or facial sweating may occur in some patients
- rarely associated with history of other chronic pain or migraine
- Autonomic symptoms
- In some patients the pain does not match with the above criteria and may have a background pain of lower intensity for 50% of the time.
- These patients are said to have “atypical trigeminal neuralgia” or “type 2”
- Patients may experience as few as three or four attacks a day but in some cases there can be as many as 70 per day.
- Aetiology
- Exact cause of trigeminal neuralgia remains unclear
- most cases are considered idiopathic
- many are associated with demyelination of the trigeminal nerve. due to:
- vascular compression of the nerve root by aberrant or tortuous vessels
- multiple sclerosis or tumours affecting the nerve root
- Imaging
- MRI is typically normal
- definable pathology
- intracranial tumours
- vascular anomalies
- ms: demyelinating plaque
- treatment
- The aim of treatment for trigeminal neuralgia is pain relief
- medical management
- carbamazepine – s/E: tiredness and poor concentration and there is a high risk of drug interactions.
- oxcarbazepine
- baclofen
- lamotrigine
- surgical management
- palliative destructive procedures
- destruction of trigeminal nerve root with the aim to relieve pain
- microvascular decompression:
- aims to decompress the trigeminal nerve
- palliative destructive procedures
Glossopharyngeal neuralgia
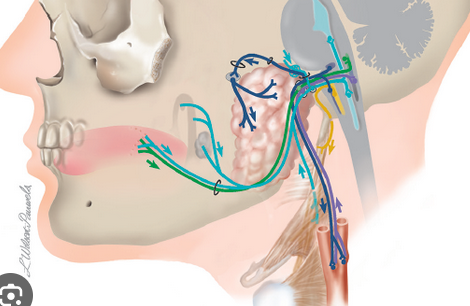
- The glossopharyngeal and fibres of the vagus nerves supply sensation to the posterior third of the tongue and oropharynx.
- Symptoms
- “sharp pain occurs when swallowing”
- severe lancing pain in the oropharynx or base of the tongue when swallowing.
- pain may be felt in the posterior mandibular region.
- The causation and quality of pain are similar to those of trigeminal neuralgia.
Facial migraine
- in the peri-orbital region, which may diffuse to the cheek and mandible.
- Management is as for typical migraine.
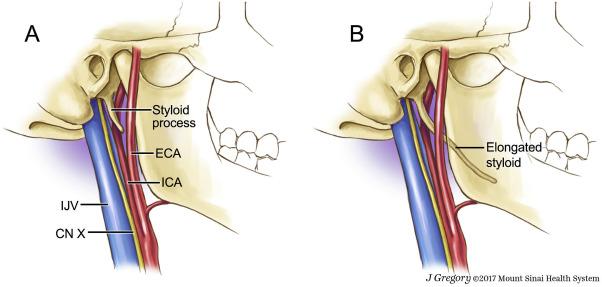
Elongated styloid process (Eagle’s syndrome)
- anatomical variant
- result from calcification of the stylohyoid ligament
- incidence of an elongated styloid process (>2.5 cm) is 4%
Symptoms
- Sharp
- occasionally bilateral
- pain when the process impinges on the soft tissues of the neck
- swallowing
- head movements
- neck tenderness at the tip of the process.
Diagnosis
- OPG
Treatment
- ultrasonic osteotomy is the treatment of choice where pain is troublesome.
Cranial (temporal) arteritis
- inflammatory disease (giant cell arteritis)
- media of medium-sized cranial arteries. It may present as
- SSx
- claudication when chewing
- constant unilateral headache
- diffuse pain around the ear
- Ix
- A temporal artery biopsy : histopathology often fails to identify a lesion in the presence of disease as ‘skip’ lesions
- Diagnosis
- presence of tenderness and hypersensitivity over the superficial temporal artery
- raised erythrocyte sedimentation rate (ESR)
- Mx
- Waiting for a positive result before commencing treatment can result in permanent ocular damage due to concurrent inflammation of the ophthalmic arteries.
- immediate commencement of oral prednisolone (commonly 50 mg daily).
- dose of prednisolone is titrated depending on ESR and clinical response
- frequently necessary to continue drug therapy for more than six months.
Temporomandibular joint dysfunction
- “a collective term embracing a number of clinical problems that involve the masticatory musculature, the Temporomandibular joint and associated structures, or both”
aetiology
- not always clear but is likely to be multifactorial
- probable causes::
- trauma from a severe blow to the jaw
- degeneration of the joint
- osteoarthritis
- rheumatoid arthritis
- displacement or dislocation of the disk
- probable contributing causal factors:
- dental malocclusion is no longer considered a causal factor
- emotional stress producing masseter spasm
- responses to stress
- anxiety
- habits that overwork the jaw muscles, such as
- parafunctional habits
- bruxism [teeth grinding]
- teeth clenching
- lip biting
- chewing on a pen
- chewing gum
- parafunctional habits
- poor posture of the head, neck and shoulders
- e.g. pushing the head forward or slouching while working at a computer – this may strain the muscular and skeletal systems that are related to the jaw muscles and joints
- probable causes::
- about 75 % of patients with TMJ disorders have a significant psychological abnormality
- e.g – anxiety and depression disorders and other emotional disturbances (2).
clinical features
- three cardinal features:
- orofacial pain
- most common presenting complain
- dull, unilateral or bilateral pain
- front of the tragus of the ear
- pain radiating to the ear, temple, cheek, and along the mandible is highly suggestive of TMD
- joint noise clicking or popping noise
- grating, grinding, or crunching – in osteoarthritis
- detected either by palpation or by a stethoscope placed over the temporomandibular joint
- restricted jaw function
- “generalised tight feeling”
- sensation that the jaw suddenly ‘catches’, ‘gets stuck’, or ‘locks’
- locking of the jaw can be – open (inability to close fully) or closed (inability to open fully)
- Other non specific features may be present:
- headache.
- earaches
- neck and shoulder pain
- tinnitus
- underlying stress, anxiety, depression (1,3)
DDx
- dental causes:
- tooth abscess
- wisdom tooth eruption
- neuralgias and neuropathic pain disorders:
- herpes zoster and postherpetic neuralgia
- trigeminal neuralgia
- mastoiditis
- otitis externa
- otitis media
- parotitis
- temporal arteriris
- trauma
- fractures
- dislocations
Investigations
- MRI : ‘gold standard’ as it shows the articular disc and its attachments graphically.
- OPG : reveals joint morphology and makes for easy comparison of the two sides
management
- Goals of the presented modalities are to:
- increase mandibular range of motion
- decrease joint and masticatory muscle pain and inflammation, an
- prevent further degenerative change in articulating tissues, including direct or indirect joint damage
- generally, the signs and symptoms of TMJ disorders improve over time with or without treatment
- about 50 % improve in one year and 85 % improve completely in three years (
- Patients presenting with pain around the ear are sometimes referred to a dentist, with a provisional diagnosis of TMJ dysfunction when aural causes are excluded. However, dental treatment is not indicated unless the above clinical findings are present.
- conservative treatments
- self-care practices
- eating soft foods
- applying ice packs
- avoiding extreme jaw movements
- stress-relieving relaxation techniques for relaxing and reducing stress
- practicing gentle jaw stretching and relaxing exercises
- medications
- NSAIDS
- muscle relaxants
- Diazepam, 5 mg, at night when muscle tenderness is present may provide relief through its skeletal muscle relaxant and anxiolytic effects.
- anti-depressants
- stabilization splints
- non-invasive, occlusal splints and occlusal adjustments work to establish balance in the occlusion and TMJs
- ultimate goal of splints and adjustments is to minimize pain in the joint and masticatory muscles by establishing stability
- splints may be used to control bruxism, which has been associated with tooth attrition, malocclusion, myofacial pain, and masticatory muscle strain, fatigue, and fibrosis
- long-term effectiveness of this therapy remains controversial
- Joint arthrocentesis
- The joint is lavaged and a steroid solution inserted
- Dilatation of the joint space and removal of the fine elements of joint destruction, together with the severing of adhesions, provides symptomatic relief in more than 70% of cases where there is no major structural change.
- However, the duration of pain relief is variable.
- Temporomandibular joint surgery
- Mx: Psychological component of facial pain