NECK MASSES in ADULTS
- All neck masses should be considered malignant until proven otherwise
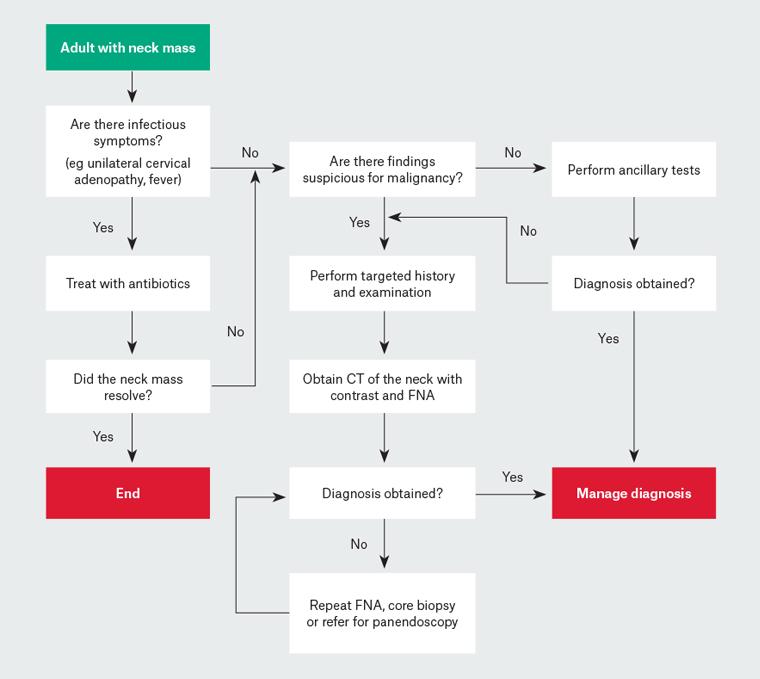
- If infectious symptoms – could treat – then need to review that has resolved
- First line investigations – CT and FNA
- Early referral ENT
- HPV associated
- In recent years, the rates of human papillomavirus (HPV)–positive oropharyngeal cancer have risen markedly, with the prevalence more than tripling from 19% to 66% between 1987 and 2006.
- The overall rate of oropharyngeal cancer is increasing despite lower rates of tobacco use
- More likely asymptomatic, cystic nodes
- Features suggestive of human papillomavirus–positive oropharyngeal cancer
- Younger age
- Male sex
- Higher number of oral and vaginal sexual partners
- Less or no tobacco exposure
- Less alcohol consumption
- Marijuana use
- Higher education
- Higher socioeconomic status
- Red flags
- Mass present > 2 weeks
- Recent voice change
- Dysphagia or odynophagia
- Ipsilateral otalgia, nasal obstruction, epistaxis
- Unexplained weight loss or loss of appetite
- Risk factors
- Smoking
- Alcohol
- Age > 40
- History of previous head and neck skin lesions
- History head or neck malignancy
- Clinical features
- Note location carefully
- Mobility – fixed more likely malignant
- Size > 1.5cm
- Firmness
- Overlying skin ulceration
- Also inspect other aspects head and neck
- Skin cancers
- Otoscopy – unilateral middle ear effusion nasopharyngeal carcinoma
- Anterior rhinoscopy
- Oral cavity, oropharynx
- Tonsil enlargement or asymmetry
- Investigations
- CT with contrast – first line to assist localize primary neoplasm
- Fine needle aspiration
- USS not first line as operator dependent – useful for guiding samples
| Ancillary investigations for adult neck massesintended to assist clinicians when malignancy is unlikely or when initial investigations do notyield a diagnosis. If these tests are undertaken, they should be based on clinical suspicion for specific diseases and should be obtained simultaneously to the malignancy work-up to prevent a delayed diagnosis. | |
| Ancillary investigation | Rationale |
| Full blood examination | Elevated white cell count may indicate infection or lymphoma |
| Anti-neutrophil antibody (ANA) | Elevated ANA may indicate autoimmune diseases |
| Erythrocyte sedimentation rate (ESR) | Elevated ESR may indicate autoimmune diseases |
| Thyroid stimulating hormone (TSH) | TSH abnormalities may indicate thyroid pathology (eg multinodular goiter, Grave’s disease) |
| Parathyroid hormone (PTH) | Elevated PTH may indicate parathyroid adenoma |
| Thyroid ultrasonography | May reveal thyroid nodules, parathyroid adenomas |
| Computed tomography of the chest with contrast | May reveal lung malignancy, tuberculosis or sarcoidosis |
| Specific infection tests (eg human immunodeficiency virus, Epstein–Barr virus, cytomegalovirus, tuberculosis) | Positive tests may indicate infectious cause |
Key points
- Head and neck malignancy is the most common cause of adult neck masses.
- It is recommended that all adult neck masses be considered malignant until proven otherwise.
- All patients presenting with a neck mass should have a thorough history taken and examination performed followed by targeted investigations.
- It is important to continue investigations until a clear and specific diagnosis has been reached.
- CT of the neck with contrast and FNA are the mainstay of investigation for all patients with a neck mass suspicious for malignancy.
- Further evaluation by an ENT specialist is required for any patient with a suspicious neck mass and normal contrast-enhanced CT of the neck.
- Ancillary testing may be performed, without delaying investigation for malignancy.
- The advice of an ENT specialist can be sought if there are any concerns or uncertainties