Haemochromatosis
Clinically important hereditary Hemochromatosis is rare
Only 10% of C282Y Homozygotes manifest disease (remainder are asymptomatic)
Cirrhosis develops in 1-2% of C282Y Homozygotes
Manifestations are twice as common and more severe in men
Etiologies
- Hereditary Hemochromatosis
- Autosomal Recessive disease (HFE Gene)
- Homozygous HFE Incidence: 1 in 250-300 caucasians
- Disrupted iron regulation results in toxic iron accumulation and tissue iron deposition
- HFE protein regulates hepcidin (iron regulatory protein)
- Hepatocytes secrete hepcidin in response to excess iron
- Hepcidin decreases intestinal iron absorption and Macrophage iron release
- Hepcidin expression is decreased in hereditary Hemochromatosis, resulting in excess iron levels
- Chromosome 6 mutations responsible
- C282Y/C282Y Mutation (90% of cases)
- The most common form of hereditary haemochromatosis (>90% of cases).
- Homozygous in 0.64% of white patients (Heterozygous in 10% – C282Y alone)
- Missense mutation with Tyrosine for cysteine at 282 on Chromosome 6
- Clinical iron overload may range from no disease to multi-organ involvement.
- Up to 50% of homozygotes do not have clinical iron overload.
- Consider serial screening of serum ferritin and transferring saturation every 1-10 years.
- C282Y/C282Y Mutation (90% of cases)
- C282Y alone
- Most of these patients have normal iron studies.
- Rarely the ferritin level is raised and in these cases it is commonly due to another cause
- Occasionally a liver biopsy may be needed to quantify hepatic iron and determine the need for treatment.
- C282Y/H63D Combination = compound heterozygote
- Combination of C282Y/H63D occurs in 2% of white patients
- These patients may have normal iron studies or mild to moderate iron overload.
- It is more common to develop severe iron overload in the setting of other causes of liver disease such as alcohol
If one parent is affected with two mutated copies (one C282Y and one H63D) for the HFE-hemochromatosis gene, and the other parent is a carrier for one H63D mutation, for each pregnancy: there is a 50% chance of inheriting one mutated copy (either one C282Y or one H63D) and one normal copy and being a carrier, and a 50% chance of inheriting two mutated copies (either two H63D copies, or one C282Y and one H63D) and being affected.
- H63D/H63D Combination
- Iron studies are usually normal. Rarely mild to moderate iron overload is seen.
- Occasionally a liver biopsy may be needed to quantify hepatic iron and determine the need for treatment.
- H63D Alone
- Iron studies are normal. If iron studies are abnormal, the
- changes are most likely to be due to another cause
- S65C Mutation
- Secondary iron overload/Raised Ferritin level
- Any Acute Inflammation
- Chronic Anemia (e.g. Thalassemia major)
- Chronic Liver Disease (e.g. Viral Hepatitis) EtOH Hepatitis, non-alcoholic steatohepatitis)
- Malignancies
- Iron Supplementation (rare with oral iron)
- Multiple transfusions
- Parenteral Iron dextran
Pathophysiology: Hereditary Hemochromatosis
- Inappropriately high intestinal iron absorption
- Only a few extra iron milligrams absorbed each day
- Iron slowly accumulates over decades
- Results in excess body iron stores
- Normal body iron stores: 4 grams
- Exceeded by age 10 in hereditary Hemochromatosis
- Tissue injury occurs when body iron 25 grams (age 30)
- Cirrhosis when body iron 30-40 grams (age 40)
- Normal body iron stores: 4 grams
- Factors that provoke expression of disease
- Male gender (women may be protected due to Menses)
- Hepatitis C
- Alcohol Abuse
- Cirrhosis risk increases 9 fold for daily Alcohol intake of more than 60g or 4 drinks
- Manifestations
- Organ iron deposition
- Iron deposits in heart, liver and Pancreas, bones and joints
- Results in Cardiomyopathy, Cirrhosis, Diabetes Mellitus and Arthritis
- Increased oxidative DNA and free radical activity
- Hepatocellular Carcinoma risk (20 fold increase risk when Cirrhosis present)
- Breast Cancer risk (variable evidence)
- Organ iron deposition
Findings: Presentations
- Classic Presentation – Bronze diabetes (late stage, rare)
- Hyperpigmented skin
- Diabetes Mellitus
- Cirrhosis
- Typical presentations
- Weakness, lethargy and Arthralgias
- Erectile Dysfunction
- Liver Function Test abnormalities
Symptoms (asymptomatic in most cases)
Symptoms usually develop between 30 and 60 years of age.
- Common symptoms
- Fatigue, Lassitude, or weakness
- Arthralgias
- Impotence
- Other symptoms
- Weight loss
- Abdominal Pain
- Hyperpigmented skin
Signs
- Brown skin pigmentation
- Hepatomegaly
- Loss of body hair
- Edema
- Ascites
- Peripheral neuritis
- Testicular atrophy
- Synovitis at second and third metacarpophalangeal joints
Complications
- Cirrhosis
- Associated 20 fold increased lifetime risk of Hepatocellular Carcinoma (4% annual Incidence)
- Hepatic encephalopathy
- Hepatorenal and hepatopulmonary syndromes
- Spontaneous bacterial peritonitis
- Variceal haemorrhage
- Diabetes Mellitus
- Arthritis (MCP joints) or Pseudogout
- Hypogonadism
- Hypothyroidism
- Restrictive Cardiomyopathy (reversible if treated before Heart Failure develops)
- Diastolic Dysfunction
- Atrioventricular Block
- Dysrhythmias
- Skin Hyperpigmentation (bronze or gray color)
- Infection
- Vibrio vulnificus
- Listeria monocytogenes
- Pasteurella pseudotuberculosis
Screening
- As HFE-haemochromatosis is an autosomal recessive disease, genetic testing of siblings and other first degree family members is recommended.
- Risk if sibling with Hemochromatosis: 25%
- Risk if parent with Hemochromatosis: 5%
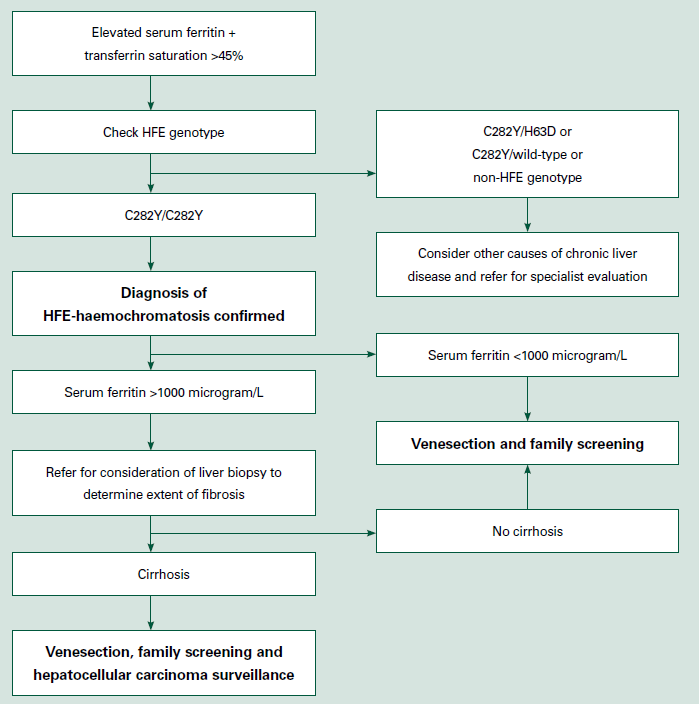
Investigations
- Patients with suspected iron overload should first have their serum ferritin and fasting transferrin saturation measured.
- Iron Saturation (Serum Transferrin Saturation)
- Fasting is no longer required as non-Fasting values are accurate
- Serum Ferritin
- Abnormal levels suggesting Hemochromatosis
- Men >250-300 ng/ml
- Women > 200 ng/ml
- Cirrhosis is unlikely when Ferritin <1000 ng/ml
- ferritin concentration is increased in
- inflammatory conditions
- chronic viral hepatitis
- nonalcoholic fatty liver disease
- alcoholic liver disease
- systemic infections (as a consequence of hepatocyte injury)
- rheumatoid arthritis
- hemophagocytic lymphohistiocytosis
- obesity
- hazardous alcohol consumption
- Metabolic (dysfunction) associated fatty liver disease (MAFLD) is frequently associated with mild to moderate elevation of serum ferritin (<1000 μg/L).
- If 1000 μg/L, secondary iron overload should be excluded by examination of the blood film
- Hemoglobinopathies (eg, sickle cell disease, thalassemia, sideroblastic anemias)
- Congenital hemolytic anemias (eg, hemoglobinopathies, hereditary spherocytosis)
- Myelodysplasia
- Increased iron absorption
- Exogenous iron given to treat anemia
- Repeated blood transfusions
- inflammatory conditions
- Abnormal levels suggesting Hemochromatosis
- Transferrin
- is the major iron transport protein in the body.
- Transferrin saturation is calculated from serum iron and transferrin concentrations and reflects altered ironmetabolism.
- In HFE the transferrin saturation is likely to be elevated (>45%) before serum ferritin increases.
- Measuring transferrin saturation after an overnight fast decreases the effect of diurnal variation of serum iron, and a value of >45% is suggestive of iron overload
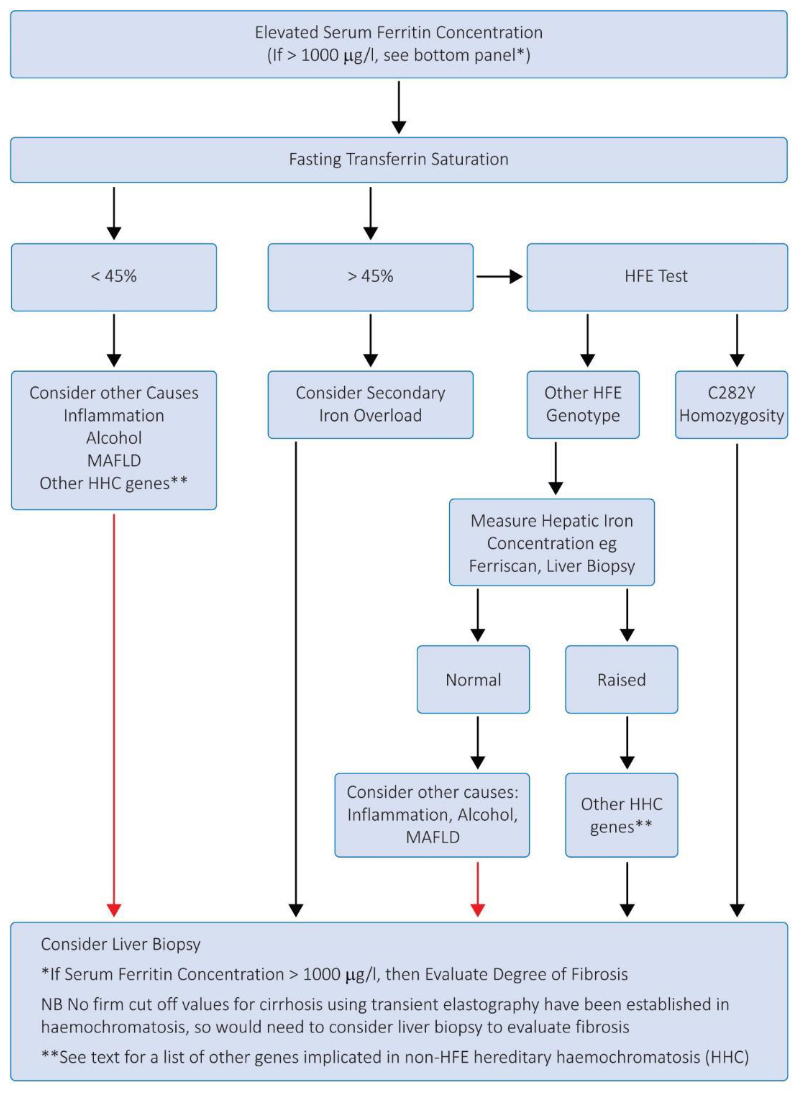
- HFE genotyping
- should be carried out in all patients with an elevated serum ferritin and transferrin saturation.
- Diagnosis of HFE-haemochromatosis should not be based on C282Y homozygosity alone, but requires evidence of increased hepatic iron stores.
- People who are C282Y homozygotes with normal iron stores should undergo regular testing.
- Compound heterozygotes (C282Y/H63D) and H63D homozygotes presenting with an elevated serum ferritin should first be investigated for other causes of an elevated serum ferritin, in particular alcohol and non-alcoholic fatty liver disease.
- Liver biopsy
- should be offered to C282Y homozygotes with a serum ferritin greater than 1000 microgram/L as these patients are at risk of cirrhosis.
- Findings
- Hepatic tissue iron index>2 (tissue iron umoles/age)
- Excessive Hemosiderin deposits
- Site of iron deposition varies per cause
- Hereditary Hemochromatosis: Hepatocytes
- Secondary iron overload: Kupffer cells
Management
- Test ALL first degree relatives
- Venesection
- Prerequisites
- haemochromatosis
- C282Y homozygosity
- C282Y/H63D compound heterozygosity
- Clinical iron overload supported by FerriScan® MRI or liver biopsy
- polycythaemia rubra vera and porphyria cutanea tarda
- (not for C282Y carrier with elevated serum ferritin and normal transferrin saturations)
- stable haemoglobin >120g/L
- serum ferritin above 25μg/L, usually above 50μg/L
- stable blood pressure systolic 110-160mmHg, diastolic 60-95mmHg
- stable pulse 50-100/minute
- haemochromatosis
- 1. Iron unloading phase, target serum ferritin ~50μg/L
- weekly venesection of ~7mL/kg (maximum 550mL) whole blood
- ensure pre-venesection haemoglobin >120g/L
- monitor haemoglobin (Hb) and serum ferritin (SF)
- Hb: is it safe to remove more blood?
- delay for 1 week if pre-venesection Hb<120 g/L
- SF: is it safe to remove more iron?
- monitor SF every 4-6 venesections, more often as SF approaches 100μg/L
- it may take many months or even years to unload excess iron
- oral supplements for vitamin B12 (5μg daily) and folate (500μg daily) support erythropoiesis during frequent venesections
- Prerequisites
- 2. Lifelong maintenance phase, target serum ferritin ~50-100 μg/L
- venesections to maintain SF ~50-100 μg/L
- highly variable between individuals, often in the range 2-6 venesections per year
- check Hb before every venesection
- monitor SF periodically – at least every 12 months, maybe every 2-6 months, highly variable
- monitoring SF is the only way to ensure safe SF levels maintained – not too high, not too low
- Possible Complications
- haematoma
- hypovolaemia
- vasovagal syncope
- venous scarring
- phlebitis
- adverse reaction to lignocaine if used
- if patient becomes tachycardic, hypotensive, restless or clammy, stop procedure and review patien
- Expected effects of phlebotomy
- Removes excess iron and normalizes tissue iron stores
- Prevents progression and complications
- Fatigue and lethargy resolve
- Skin bronzing improves
- Cardiac function and Restrictive Cardiomyopathy improve
- Hepatomegaly and Liver Function Test abnormalities improve (hepatic fibrosis improves in 30% of cases)
- However, Diabetes Mellitus control may be unaffected
- Dietary recommendations
- Avoid Hepatotoxins including Alcohol
- no requirement for a low iron diet in the management of HFE as venesection is so effective in removing excess iron stores. However, it is reasonable for patients to choose to reduce red meat intake if they wish to do so (e.g., to approximately 90-120 g/day), as this may reduce the frequency of venesections.
- Vitamin C (ascorbic acid) supplements should be avoided since vitamin C can increase iron absorption and iron toxicity.