Hydrocele
- is an abnormal collection of serous fluid between the two layers of tunica vaginalis of testis.
- Primary hydrocele
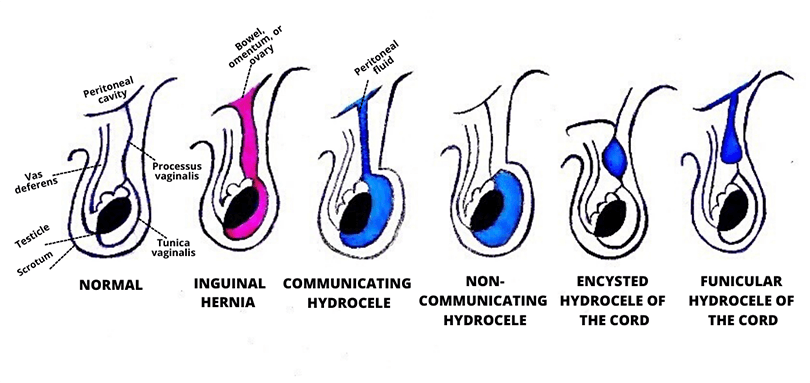
- Congenital Hydrocele:
- failure of processus vaginalis to obliterate and remains patent and results in free communication with the peritoneal cavity, leading to congenital hydrocele.
- Infantile Hydrocele:
- In this case, processus vaginalis gets obliterated at the level of the deep inguinal ring. However, the portion distal to it remains patent and allows fluid accumulation.
- Encysted Hydrocele of the Cord:
- Both the proximal and distal portions of processus vaginalis get obliterated while the central portion remains patent and fluid accumulates within it.
- Vaginal Hydrocele:
- Processus vaginalis remains patent only around the testes, and, as fluid accumulates, it renders the testes impalpable.
- Secondary/Acquired:
- infection (filariasis, tuberculosis of the epididymis, syphilis)
- injury (trauma, post-herniorrhaphy hydrocele),
- malignancy
(This type of hydrocele tends to be small, with the exception of secondary hydrocele due to filariasis, which can be very large)
Etiology
- Connection with the peritoneal cavity through a patent processes vaginalis (congenital).
- Excessive production of fluid (secondary hydrocele).
- Defective absorption of fluid.
- Interference with the lymphatic drainage of scrotal structures as in filarial hydroceles.
- In children, patency of processus vaginalis, allowing peritoneal fluid to flow into the scrotum, is the main cause of hydrocele.
- However, in adults, filariasis caused by Wuchereria bancrofti is the main culprit globally, affecting 120 million people in more than 73 countries
- In Australia – iatrogenic causes (either trauma or post-herniorrhaphy complications) predominate
History and Physical
- painless scrotal swelling
- testes impalpable
- positive transillumination and fluctuation.
- Congenital hydrocele tends to be intermittent as it usually reduces when lying flat due to drainage of hydrocele fluid into the peritoneum. However, applying pressure on the congenital hydrocele does not reduce it.
Examination:
- Is it possible to reach above the swelling and palpate the cord?
- If no, this could represent a hydrocele (congenital or infantile) or a hernia.
- A hernia can be differentiated from hydrocele in terms of having expansile cough impulse and reducibility but lacking transillumination and fluctuation.
- Does the swelling arise from testis or epididymis or encase both of these structures.
- Hydroceles tend to surround both testes and epididymis, rendering them impalpable.
- Does the swelling transilluminate?
differential diagnosis.
- Inguinal Hernia:
- Laboratory tests are usually not indicated,
- but in the case of an incarcerated inguinal hernia, which can mimic hydrocele, leukocytosis can aid in the differentiation.
- Negative transillumination and palpable bowel at the deep ring on the digital examination is more consistent with an inguinal hernia.
- Testicular Tumor:
- Serum alpha-fetoprotein and human chorionic gonadotropin (hCG) levels are indicated if there is suspicion of malignant teratomas or other germ cell tumors.
- Epididymitis/Orchitis:
- These conditions can lead to secondary or reactive hydroceles.
- In such cases, urinalysis and urine culture may be useful.
- Imaging Studies
- USS – evaluating hydrocele + underlying processes such as epididymitis, testicular torsion,testicular tumor, Spermatoceles, and testicular atrophy
Treatment / Management
- Surgery is the treatment of choice for hydrocele, and it is warranted when hydrocele becomes complicated or symptomatic.
- Complications of Surgery
- Reactionary hemorrhage
- Pyocele
- Infection
- Sinus formation
- Recurrent hydrocele
- Complications of Surgery
- Prognosis
- Congenital hydroceles tend to resolve spontaneously by the end of the first year of life.
- In experienced hands, hydrocele repair carries a very low risk of testicular damage or recurrence.
- The prognosis of the adult-onset hydrocele is mainly dependent on the underlying cause. For instance, filarial hydrocele’s prognosis depends on its size and the severity of lymphatic obstruction.
- Complications are attributable to the pathology itself and the treatment administered
- Infection
- Pyocele
- Haematocele
- Atrophy of testes
- Infertility (resulting from the spermatogenesis halt due to increased pressure on the blood supply on the testis from edema)
- Ruptur
- Hernia of hydrocele (rare)