Premature ejaculation
- Premature ejaculation is the most common cause of sexual dysfunction, especially in the younger age group.
- It is estimated that premature ejaculation affects up to 31% of Australian males.
- Premature ejaculation causes significant psychological, emotional and interpersonal distress for the patient and his partner.
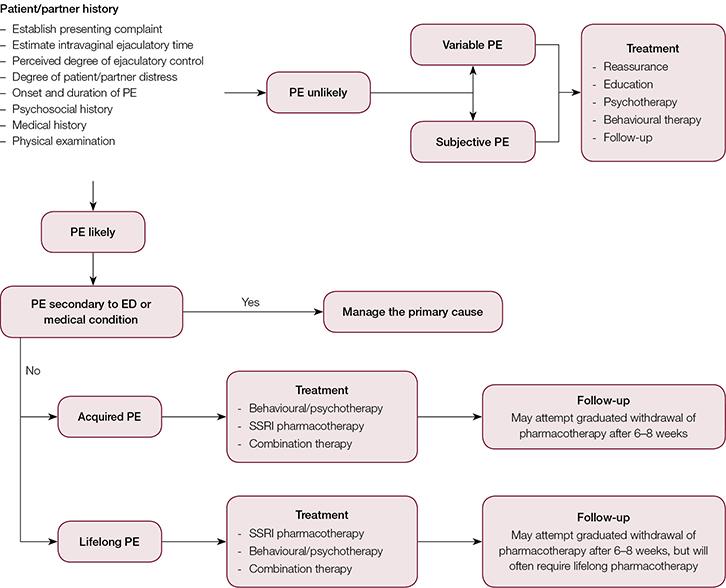
- Premature ejaculation can be lifelong (primary) or acquired (secondary), and this distinction guides management.
- Primary or secondary(more common)
- Primary – no other underlying cause, usually requires pharmacological
- intravaginal ejaculatory latency time (IELT) = the time from vaginal penetration to ejaculation.
- Lifelong premature ejaculation – IELT of <1 minutes since first intercourse
- acquired premature ejaculation – IELT of <3 minutes at any point in a man’s life
- Premature ejaculation can be further divided into authority-based subtypes ‘variable’ and ‘subjective’ – which describe individuals experiencing significant distress and dissatisfaction with ejaculation
|
|
Lifelong (primary) |
Acquired (secondary) |
Variable |
Subjective |
|
IELT criteria |
<1 minute |
<3 minutes |
Short or normal |
Normal or prolonged |
|
Symptoms |
Ejaculation occurs too early in nearly every sexual encounter |
New onset of premature ejaculation, usually the result of an identifiable source and patient has experienced normal ejaculations in the past |
PE is inconsistent and occurs irregularly and not the result of (psycho)pathology |
Subjective, self- perception of rapid ejaculation despite normal ejaculation time |
|
Onset |
Early, usually from first sexual encounter |
Can occur at any time in a man’s life |
Can occur at any time in a man’s life |
Can occur at any time in a man’s life |
|
Prevalence |
Low |
Low |
High |
High |
|
Quality of ejaculation control |
Ejaculation remains rapid throughout lifetime with no ability to control ejaculation |
Ability to delay ejaculation may be diminished or lacking |
Ability to delay ejaculation may be diminished or lacking |
Ability to delay ejaculation may be diminished or lacking |
|
Aetiology |
Genetic Neurobiological |
Urological (erectile dysfunction, prostatitis) Hormonal (hyperthyroidism) Psychological Relationship problems |
Normal variance of sexual performance |
Psychological preoccupation with imagined rapid ejaculation |
|
Treatment |
Pharmacotherapy Psychotherapy +/– |
Medical management Pharmacotherapy Psychotherapy Education |
Reassurance Education Behavioural therapy |
Psychotherapy Reassurance Education |
Treatment
- Behavioural therapy
- stop-start” – ceased genital stimulation until heightened arousal sensation subsides AND “squeeze” – where the glans prepuce is squeezed at heightened arousal
- Extended foreplay
- Pre-intercourse masterbation
- Alternate positions
- Interval sex
- Increased frequency
- Psychosexual counselling – address the issues anxiety/psychogenic cause
Medications
- SSRIs
- Dapoxetime 30mg 1-3 hours before intercourse- short acting SSRI – expensive
- Fluoxetine, paroxetine, sertraline regualrly
- PDE-5 inhibitiors if related to ED
- Reducing penile sensation
- topical applications
- condoms
|
Agent |
Recommended dose |
Half-life (hrs) |
IELT fold increase |
Adverse effects |
Additional notes |
|
Dapoxetine (SSRI) – short acting |
30–60 mg, 1–3 hours before intercourse |
1.5 |
2.5–3
|
Nausea, diarrhoea, headache, somnolence, dizziness |
TGA approved, not currently on PBS No significant drug–drug interactions Effective treatment for both acquired and lifelong PE |
|
Paroxetine (SSRI) |
10–40 mg/day and 20 mg, 3–4 hours prior to intercourse |
21 |
11.6 |
Insomnia, anxiety, nausea, loss of libido, ED, anhidrosis |
Off-label prescriptions Used for lifelong and acquired PE Therapeutic effect achieved in 2–3 weeks May hinder sperm motility May induce mania in bipolar patients On-demand use not as effective without daily regimen |
|
Fluoxetine (SSRI) |
20–40 mg/day |
36 |
5 |
Insomnia, anxiety, nausea, loss of libido, ED, anhidrosis |
|
|
Sertraline (SSRI) |
50–200 mg/day and 50 mg, 4–8 hours prior to intercourse |
26 |
5 |
Insomnia, anxiety, nausea, loss of libido, ED, anhidrosis |
|
|
Clomipramine (TCA) |
12.5–50 mg/day and 25 mg, 4–24 hours prior to intercourse |
19–37 |
6 |
Nausea, dry mouth, ED, hot flushes, arrhythmias |
|
|
Tramadol |
25–50 mg, 3–5 hours prior to intercourse |
5–7 |
4–7.3 |
Nausea, dizziness, insomnia, dyspepsia, seizures |
Possible opioid addiction TCAs and SSRIs are contraindicated with Tramadol use Multiple drug interactions-only indicated as monotherapy in refractory PE |
|
Phosphodiesterase-5 inhibitors |
25–100 mg, 30–50 minutes prior to intercourse |
3–6 |
Monotherapy has no effect on IELT |
Headache, flushing, dyspepsia |
Used for concomitant ED and PE Improved efficacy when combined with SSRI therapy Not established monotherapy for PE |
|
Prilocaine-lignocaine topical cream/aerosols |
2.5 g, applied 20–30 minutes prior to intercourse |
1–2 |
4–6 |
ED, loss of sensation in penis and partner’s vagina, skin irritation |