Testicular/scrotal abnormalities
| Signs and symptoms in the classic case | ||
| Symptoms | Signs | |
| Testicular torsion | Sudden onset Severe pain Associated nausea and vomiting Associated trauma Possible abdominal pain | Asymmetric, high-riding testis Negative Prehn’s sign Absent cremasteric reflex |
| Epididymitis | Insidious onset Fevers and rigors Lower urinary tract symptoms Relevant sexual history | Indurated testis Tender upper pole of testis Positive Prehn’s sign Intact cremasteric reflex |
| Torsion of the appendix testis | Gradual onset Moderate to severe pain Associated nausea and vomiting | Localised tenderness to anterior testis‘ Blue dot’ sign |
Non-painful scrotal swelling
| Hydrocele | Varicocele | Idiopathic scrotal oedema | Tumour/ leukaemia | |
| Typical age group | Infants | Peri-pubertal | 3-7 years | 1-8 years |
| Fever | Unusual | Unusual | Unusual | Possible |
| Palpation | Soft Non-tender Fluctuant | “Bag of Worms” Occasionally tender | Non-tender May have low-grade discomfort | Hard Non-tender May be painful if rapidly growing |
| Swelling pattern | Scrotal | Predominantly left-sided | Can extend across midline and into perineum, groin, penis | Unilateral or bilateral |
| Discoloration | No | No | Bland, purplish | No |
| Transilluminable | Brightly | No | No | No |
| Reactive hydrocele | – | No | No | Possible |
Scrotal pain +/- swelling
| Testicular torsion | Irreducible hernia | Torsion of testicular appendage | Epididymo-orchitis | Trauma eg testicular or epididymal rupture | |
| Typical age group | Pubertal (and rarely neonates) | Infants | Pre-pubertal (7-12 years) | <2 years and post-pubertal (rarely pre-pubertal) | – |
| Pain | Severe Usually sudden onsetMay radiate to iliac fossa or thigh | Irritable | Usually sudden onset Usually minimal at rest | Sudden or subacute onset May improve with elevation | May be delayed |
| Swelling | Yes | Yes May extend to scrotum | Yes | Yes | May be delayed |
| Fever | Unusual | Unusual | Unusual | Common | Unusual |
| Nausea and vomiting | Common (90%) | Common | Uncommon | Uncommon | Uncommon |
| Dysuria or discharge | No | No | No | Common | No |
| Gait | Impaired | – | – | – | – |
| Position of testis | High riding or horizontal | – | Normal | – | – |
| Palpation | Tender Thickened spermatic cord | Firm and tender Swelling not reducible | Focal tenderness of upper pole of testis | Tender postero-lateral testis | Tender |
| Oedema crosses midline | No | No | No | Possible | Possible |
| Discoloration | Red/blue Dark in neonate | – | Blue dot sign | Red | Bruising(consider causes, eg NAI) |
| Cremasteric reflex | Usually absent | Usually present | Usually present | Usually present | Usually present |
| Reactive hydrocele | Possible | No | No | Possible | Possible |
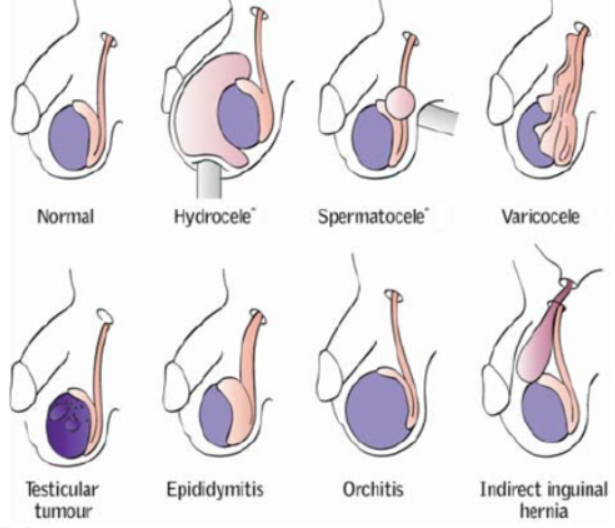
Testicular lump differentials
- Average testicular weight 20 g, > 15mL (< 12mL is reduced)
- Intratesticular:
- malignant testicular tumour
- Painless, may have dull ache heaviness, firmness or swelling
- benign intratest lesions:
- simple cyst
- epidermoid cyst
- benign teratoma (esp in prepubertal testis)
- malignant testicular tumour
- Inflammatory:
- acute epidiymoorchitis
- Most common cause painful swelling in post-pubertal males
- Infection due to Chlamydia ro Gonorrhea < 35 years
- E coli > 35
- If severe can cause scrotal swelling, urethral discharge, pain, fevers, LUTS
- Elevation of scrotum
- viral orchitis
- Swelling/pain in on or both testicles
- Usually due to infection
- Testis is enlarge, indurated, tender on palpation
- Treatment – bed rest, ice, scrotal support, analgesia, treat infection
- chronic tuberculous epididymoorchitis
- schistosomal epididymitis
- sperm granuloma
- acute epidiymoorchitis
- Traumatic:
- scrotal haematoma
- haematocele: haematoma w/in TV
- testicular haematoma: haematoma w/in TA
- Derangement of testicular, adnexal or cord anatomy:
- epididymal cysts or spermatocele of the epididymis
- Fluid filled cyst that develops at the head of the epididymis
- Generally painless
- Usually filled with mild fluid and may contain sperm
- varicocele: varicosities of the pampiniform plexus
- Tortuosity
- Present in up to 20% of males
- Often asymptomatic
- Most common surgically correctable cause of infertility
- inguinal hernia: patent processus vag in children (–> indirect)
- hydrocele:
- Painless scrotal swelling which tends to worsen throughout the day
- Collection of peritoneal fluid between the parietal and visceral layers of the tunica vaginalis
- late (missed) or prenatal torsion of the spermatic cord
- persistence of embryological vestigular structures:
- Müllerian duct remnant (appendix testis)
- Wolffian duct remnants (appendix epididymis, vas aberrans of Haller, paradidymis)
- epididymal cysts or spermatocele of the epididymis
- Miscellaneous:
- acute idiopathic scrotal oedema
- cutaneous lesions (e.g. sebaceous cysts)
- Henoch-Schönlein purpura
- Testicular torsion
- Sudden onset pain, ischaemia, assymetrical