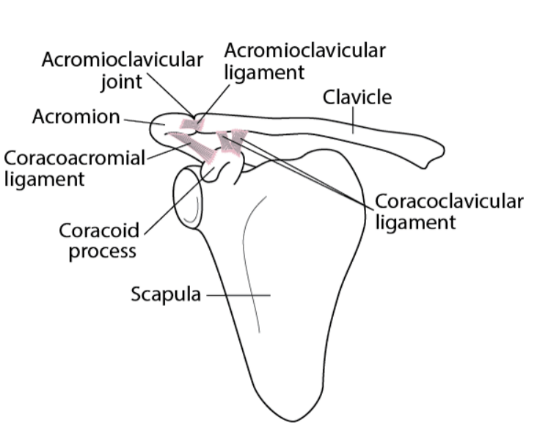
Acromioclavicular joint sprain
- Several ligaments surround this joint and, depending on the severity of the injury, one or all of the ligaments may be torn. Severe sprains tear the acromioclavicular and coracoclavicular ligaments.
- The acromioclavicular joint is commonly injured when the clavicle is fractured.
- Patients have pain and tenderness at the acromioclavicular joint
Clinical assessment
- Point tenderness over the ACJ is very typical with either an ACJ sprain or osteoarthritis.
- O’Brien test
- sensitivity of 16–100%
- specificity of 90–96.6% – highly suggestive of localised ACJ pathology, most often a sprain or osteoarthritis.
- superficial pain localized to AC joint is suggestive of AC joint pathology
- deep pain is suggestive of a SLAP lesion
Investigations
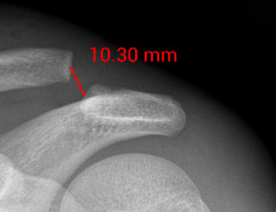
Xray:
- soft tissue swelling/stranding
- widening of the acromioclavicular joint
- normal: 5-8 mm (narrower in the elderly)
- greater than 2-4 mm asymmetry (compared to radiographs of the contralateral side)
- increased coracoclavicular distance
- normal: 10-13 mm
- greater than 5 mm asymmetry (compared to the contralateral side)
- superior displacement of the distal clavicle
- the inferior edge of the acromion should be level with the inferior edge of the clavicle
 |  |
 |
Referral and management
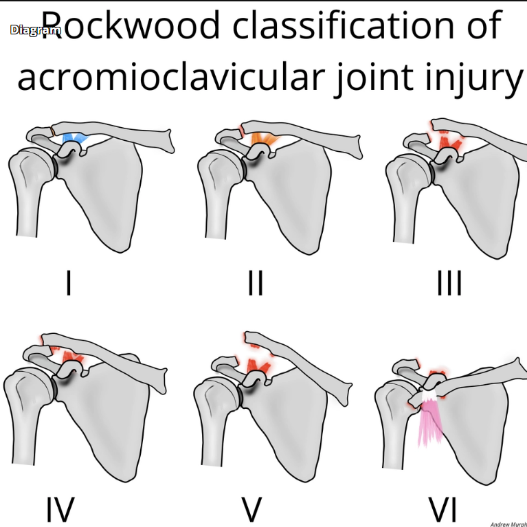
| Type | AC ligament | CC ligament | Exam | Radiographs | Reducibility | Treatment |
| Type I | Sprain | Normal | AC tendernessNo AC instability | Normal | Reducible | Sling |
| Type II | Torn | Sprain | AC horizontal instability | AC joint disruptedIncreased CC distance < 25% of contralateral | Reducible | Sling |
| Type III | Torn | Torn | AC joint disruptedIncreased CC distance 25-100% of contralateral | Reducible | Controversial | |
| Type IV | Torn | Torn | Skin tentingPosterior fullness | Lateral clavicle displaced posterior through trapezius on the axillary lateral XR | Not reducible | Surgery |
| Type V | Torn | Torn | Severe shoulder droop, does not improve with shrug | Increased CC distance > 100% of contralateral | Not reducible | Surgery |
| Type VI | Torn | Torn | Rare; Associated injuries; paresthesias | Inferior dislocation of lateral clavicle, lying either in subacromial or subcoracoid position | Not reducible | Surgery |
- brief sling immobilization, rest, ice, physical therapy for type I and II
- good results when clavicle displaced < 2cm
- rehab
- early shoulder range of motion
- regain functional motion by 6 weeks
- return to normal activity at 12 weeks
- consider corticosteroid injections Supportive shoulder strapping provides ACJ stability, reduces pain and is easy to corticosteroid injected into the ACJ using an aseptic technique