Back Pain
- Without findings suggestive of serious pathology, imaging is not indicated in patients with acute low back pain.
- NSAIDS, Paracetamol, and muscle relaxants are effective treatments for nonspecific acute low back pain.
- Patient education that includes advice to
- stay active
- avoid aggravating movements
- return to normal activity as soon as possible
- discussion of the often benign nature of acute low back pain is effective in patients with nonspecific pain.
- Although regular exercises may not be beneficial in the treatment of nonspecific acute low back pain, physical therapy (McKenzie method and spine stabilization) may lessen the risk of recurrence and need for health care services.
- Spinal manipulation and chiropractic techniques are no more beneficial than established treatments for nonspecific acute low back pain, and their addition to established treatments does not improve outcomes.
- Bed rest is not helpful for nonspecific acute low back pain.
Low back pain (LBP)
- can be classified as
- Acute: Less than 4 weeks
- Subacute: 4 to 12 weeks
- Chronic: More than 12 weeks
- 90% of patients recover from an acute period of LBP, recurrences are common.
- 32% of patients with back pain will not return to work at one month
- this cohort is at risk for long-term work absence.
- stratify patients into
- red flags
- nature of pain
- non-spinal
- radicular (neuralgia due to an irritation of the sensory root or the dorsal root ganglion (DRG) of a spinal nerve)
- non-organic
- central LBP
- Patients will often present with features of multiple categories, and priority is given to ruling out sinister causes first.
- Red flags are common in patients with acute low back pain and do not necessarily indicate serious pathology
| Differential Diagnosis of Acute Low Back Pain | |
| Diagnosis | Key clinical clues |
| Intrinsic spine | |
| Compression fracture | – History of trauma (unless osteoporotic) – point tenderness at spine level – pain worsens with flexion, and while pulling up from a supine to sitting position and from a sitting to standing position |
| Herniated nucleus pulposus | – Leg pain is greater than back pain and worsens when sitting – pain from L1-L3 nerve roots radiates to hip and/or anterior thigh – pain from L4-S1 nerve roots radiates to below the knee |
| Lumbar strain/sprain | – Diffuse back pain with or without buttock pain – Pain worsens with movement and improves with rest |
| Spinal stenosis | – Leg pain is greater than back pain -pain worsens with standing and walking – pain improves with rest or when the spine is flexed – pain may be unilateral (foraminal stenosis) or bilateral (central or bilateral foraminal stenosis) |
| Spondylolisthesis | – Leg pain is greater than back pain – pain worsens with standing and walking – pain and improves with rest or when the spine is flexed – pain may be unilateral or bilateral |
| Spondylolysis | – Can cause back pain in adolescents, although it is unclear whether it causes back pain in adults – pain worsens with spine extension and activity |
| Spondylosis (degenerative disk or facet joint arthropathy) | – Similar to lumbar strain – disk pain often worsens with flexion activity or sitting – facet pain often worsens with extension activity, standing, or walking |
| Systemic | |
| Connective tissue disease | – Multiple joint arthralgias, fever, weight loss, fatigue, spinous process tenderness, other joint tenderness |
| Inflammatory spondyloarthropathy – Ankylosing spondylitis – Psoriatic spondylitis – Reiter syndrome | – Intermittent pain at night – morning pain and stiffness – inability to reverse from lumbar lordosis to lumbar flexion |
| Malignancy – Multiple myeloma – Metastatic carcinoma – Lymphoma and leukemia – Spinal cord tumors – Retroperitoneal tumors – Primary vertebral tumors | Pain worsens in prone positionspinous process tenderness, recent weight loss, fatigue |
| Infection – Osteomyelitis – Septic diskitis – Paraspinous abscess – Epidural abscess | – Constant pain – spinous process tenderness – elevated ESR and/ or C-reactive protein level |
| Referred | |
| Abdominal aortic aneurysm | Abdominal discomfortpulsatile abdominal mass |
| GI : pancreatitis, peptic ulcer disease, cholecystitis | Abdominal discomfortnausea\vomiting, symptoms often associated with eating |
| Herpes zoster | Unilateral dermatomal pain, often allodyniavesicular rash |
| Pelvic conditions: PID, Prostatitis, Endometriosis | Discomfort in lower abdomen, pelvis, or hip |
| Retroperitoneal conditions: renal colic, pyelonephritis | Costovertebral angle pain, abnormal urinalysis results, possible fever |
| Red Flags for Serious Etiologies of Acute Low Back some red flags are more important than others, and that red flags overall are poor at ruling in more serious causes of low back pain patients with back pain in the primary care setting (80%) tend to have one or more red flags, but rarely have a serious condition. However, physicians should be aware of the signs and symptoms of cauda equina syndrome, major intra-abdominal pathology, infections, malignancy, and fractures Strong vs Weak Red Flags: Presence of any strong red flag warrants more urgent workup and probable referral to a spine subspecialist. Presence of one or two weak or intermediate red flags may warrant observation because few patients will be significantly harmed if diagnosis of a serious cause is delayed for four to six weeks. | ||
| Possible etiology | History findings | Physical examination findings |
| Cancer | Strong: – Cancer metastatic to bone Intermediate: – Unexplained weight loss Weak: -Cancer – pain increased or unrelieved by rest – Night pain | Weak: – Vertebral tenderness, limited spine range of motion |
| Cauda equina syndrome | Strong: – Bladder or bowel incontinence – urinary retention – progressive motor or sensory loss | Strong: -Major motor weakness or sensory deficit – Loss of anal sphincter tone – Saddle anesthesia Weak: – Limited spine range of motion |
| Fracture | Strong: – Significant trauma related to age * Intermediate: – Prolonged use of steroids Weak: – Age older than 70 yearshistory of osteoporosis | Weak: – Vertebral tenderness – limited spine range of motion |
| Infection | Strong: – Severe pain and lumbar spine surgery within the past year Intermediate: – Intravenous drug use – Immunosuppression – Concomitant infection – severe pain and distant lumbar spine surgery Weak: -Pain increased or unrelieved by rest | Strong: Fever urinary tract infection wound in spine region Weak: Vertebral tenderness, limited spine range of motion |
| NOTE: *—Fall from a height or motor vehicle crash in a young patient, minor fall or heavy lifting in a patient with osteoporosis or possible osteoporosis. | ||
| YELLOW FLAG INDICTORS | ||
| Work | ||
| belief that pain is harmful, resulting in fear avoidance behaviour belief that all pain must be abolished before attempting to return to work or normal activity expectation of increased pain with activity or work fear of increased pain with activity or work belief that work is harmful poor work history unsupportive work environment | ||
| Beliefs | ||
| catastrophising, thinking the worst misinterpreting bodily symptoms belief that pain is uncontrollable poor compliance with exercise expectation of ‘techno-fix’ for pain low educational background | ||
| Behaviours | ||
| passive attitude to rehabilitation use of extended rest reduced activity with significant withdrawal from activities of daily living avoidance of normal activity impaired sleep because of pain increased intake of alcohol or similar substances since the onset of pain | ||
| Affective | ||
| depression feeling useless and not needed irritability anxiety about heightened body sensations disinterest in social activity over protective partner/spouse socially punitive partner/spouse lack of support to talk about problems | ||
pain history
- Circumstances associated with pain onset
- Primary site of pain
- Radiation of pain
- Character of pain (eg. is pain throbbing, sharp, aching)
- Intensity of pain (eg. on visual analogue scale)
– at rest
– on movement
– at present
– during past week
– highest level - Factors altering pain
– what makes it worse?
– what makes it better? - Associated symptoms (eg. nausea)
- Temporal factors
– is pain present continuously or otherwise? - Effect of pain on activities
- Effect of pain on sleep
- Medications taken for pain
- Other treatments used for pain
- Health professionals consulted for pain treatment
Pain history information of significance for symptomatic treatment of pain
- Expectations of outcome of pain treatment
- Patient’s belief concerning the causes of pain
- Reduction in pain required to resume reasonable activities
Patient’s typical coping response for stress - or pain, including presence of anxiety or psychiatric disorders (eg. depression or
psychosis) - Family expectations and beliefs about pain, stress and postoperative course
- Ways the patient describes or shows pain
- Patient’s knowledge, expectations and preferences for pain treatment
Physical examination
Convention dictates that the orthopaedic paradigm of:
- inspection – ‘look’
- movement ‘move’, and
- palpation ‘feel’
- While this process allows a description of the patient, current best evidence is that no particular clinical sign or combination of clinical signs elicited on physical examination allows any valid anatomical or pathological diagnosis to be applied. Nor do they offer any predictive value in terms of treatment (Australian Acute Musculoskeletal Pain Guidelines Group.Evidence based management of acute musculoskeletal pain.National Health and Medical Research Council (NHMRC), 2003.)
- Nonetheless, it has been shown that such an examination does instil confidence in the patient, from which, a simple yet effective and evidence based management plan can be invoked by an equally confident GP. Furthermore, it does provide some objectivity in terms of patient progress
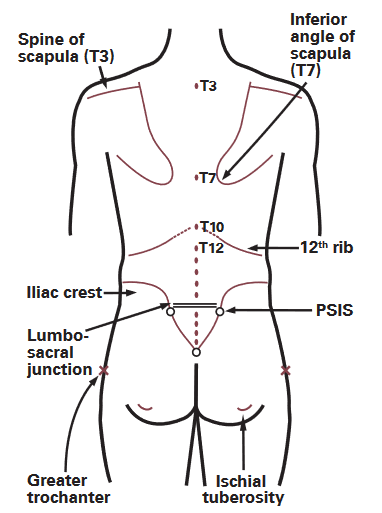
Surface anatomy landmarks
- Functional Assessment
- walking on toes (predominantly an S1 nerve root function)
- walking on heels (predominantly L5)
- getting down to and rising from the squatted position or a low chair or couch
- marking time
- walking heel-to-toe and balancing on one leg
- Inspection
- Asymmetry of posture
- spinal curves, or muscle bulk
- abnormalities on the skin.
- The level of the iliac crests is then
- thoraco-lumbar scoliosis
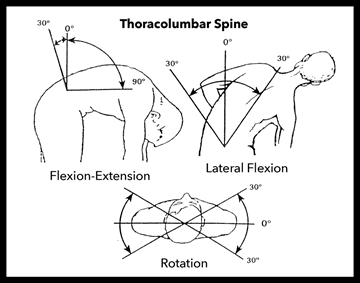
- Movement
- Flexion
- extension
- lateral flexion
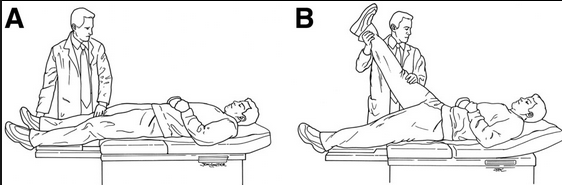
Straight leg raise
- Perform in two positions
- Supine
- Sitting
- Technique: Flex hip from 180 to 90 degrees
- Result:
- Sciatic Pain at 30 to 70 degrees
- Aggravation of pain with dorsiflexion of the foot
- Relief of pain by knee flexion
- Observe discrepancy between supine and sitting SLR: Discrepancy suggests Malingering
- Predicting Lumbar Disc Herniation
- Test Sensitivity: 80-98%
- Test Specificity: 40-60%

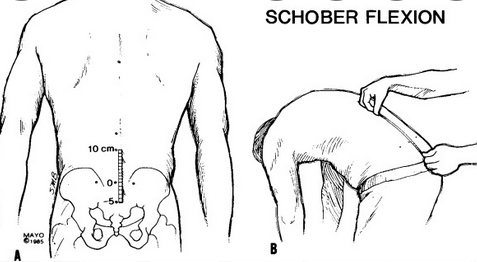
Schobers
- Positive Schober’s Test: Less than 5cm increase in length with forward flexion: Decreased lumbar spine range of motion, ankylosing spondylitis
L neuro exam
- Gait – high stepping (foot drop)
- Motor and Sensory Exam
- Reflexes
- Deep Tendon Reflexes
- Hyperactive reflexes with abnormal Babinski : Suggests Bilateral pyramidal tract dysfunction
- spinal Cord Compression
- Cervical Spondylosis
- Tumor
- Central DIsc Herniation
- Hypoactive reflexes
- Bilateral
- Normal
- Spinal Shock
- Myopathy
- Bilateral
- Unilateral: Peripheral Nerve
- Ankle (S1)
- Knee (L3,L4)
- Hyperactive reflexes with abnormal Babinski : Suggests Bilateral pyramidal tract dysfunction
- Deep Tendon Reflexes
- L5 lesion:
- Weakness in hip extension, knee flexion, dorsi flexion, inversion, eversion
- EDB – extensors of toes (get wasting too)
- Intact reflexes
- Sensory: lat leg, dorsum of foot
- S1 lesion:
- Weakness in hip extension, knee flexion, plantar flexion, eversion and inversion
- Absent ankle jerks
- Reduced sensation lateral side of foot
| Neurologic Examination Findings in Patients with Acute Low Back Pain | ||||||
| affectednerve root | motor deficit | sensory deficit | reflex | disk herniation | ||
| central | paracentral | lateral | ||||
| L3 | Hip flexion | Anteriormedial thigh | Patella | Above L2-L3 | L2-L3 | L3-L4 |
| L4 | Knee extension | Anterior legmedial foot | Patella | Above L3-L4 | L3-L4 | L4-L5 |
| L5 | Dorsiflexiongreat toe | Lateral legdorsal foot | Medial hamstring | Above L4-L5 | L4-L5 | L5-S1 |
| S1 | Plantar flexion | Posterior leg/lateral foot | Achilles tendon | Above L5-S1 | L5-S1 | None |
Nonorganic signs of LBP
- Widespread ‘nonanatomical’ tenderness and/or superficial tenderness
- Back pain on simulated tests for axial loading
- Back pain on simulated rotation of the hips
- Straight leg raise improves with distraction
- Regional sensory changes (nondermatomal)
- Regional weakness (jerky, give way weakness in nonanatomical distribution)
- Over reaction during examination (overt pain behaviour, eg. crying out, exaggerated responses
Investigations
- Imaging
- Not recommended for routine Low Back Pain in the first 6 weeks
- Obtain for Low Back Pain Red Flag symptoms
- Obtain when surgery is being considered
- The decision to order spinal imaging in primary care is likely to be influenced by the patient, clinician and systemic factors.
- Ex: general practitioners and their patients are likely to be eager to obtain
- a specific diagnosis
- ascertain treatment option
- rule out a serious underlying cause.
- particularly important to clinicians who perceive themselves as vulnerable to litigation and are challenged by the need to exclude the possibility of serious pathology within short consultation times.
- Even in situations where the GP advises against imaging, patient expectations (along with GP perceptions of the expectations of their patients) may nonetheless lead to referral.
- In Australia, spinal imaging is widely available and easily organised via an abundance of private radiology companies
- As a result, imaging is frequently expected by patients and preferred by clinicians. highly accessible
- imaging may have adverse effects via psycho-behavioural mechanisms
- spinal imaging for NSLBP has been found to be associated with increased or prolonged disability, increased healthcare costs and a decreased sense of wellbeing
- this is due to radiologists often report an array of abnormalities, which frequently fall within the range of age-related norms.
- Many common degenerative features are present in asymptomatic populations and are not robustly linked to clinical symptoms and long-term individual outcomes.
- Spinal imaging is often reported in a manner that leads to misunderstanding of the relevance of the features identified, leading patients to believe that their spine is ‘damaged’ or vulnerable – perhaps irreversibly.
- These negative structure-related perceptions and beliefs may in turn lead to distress, enhanced pain via neuropsychological and neuro-immune mechanisms, and the compounding of disability through behavioural mechanisms such as fear and avoidance.
- Ex: general practitioners and their patients are likely to be eager to obtain
- OPTIONS
- Lumbosacral Spine XRay
- Lumbar Spine MRI (Most accurate)
- Lumbar Spine CT (Less accurate than MRI)
- Spine Bone Scan
- Important messages for patient–clinician interactions
- Without clinical risk factors (red flags), serious pathology is uncommon.
- Positive communication from the clinician has a significant impact on the patient.
- Most non-specific low back pain improves after 4–6 weeks, and returning to normal activity as soon as possible is highly beneficial.
- Evidence shows no benefit (and potentially negative impact) of routine imaging.
- When imaging is expected, discussions of evidence-based guidelines to aid in education may prove helpful.
- Radiological abnormalities are common and not often correlated with clinical presentation.
- Imaging findings including ‘age-related changes’ should be explained to the patient with epidemiological context and with non-threatening language.
- Referral to other health professionals may aid in patient education and improved recovery.
Treatment
| recommendations for treating chronic low back pain | ||
| First-line treatment | Second-line treatment | Third-line treatment |
| Education Early return to activity Weight loss Exercise/physiotherapy Nonsteroidal anti-inflammatory drugs Tai chi/yoga/Pilates Paracetamol Acupuncture | Multidisciplinary rehabilitation Psychological therapy Antidepressants (onsider as first-line treatment if patient has chronic back pain and depression) Injections – facet/epidural | Tapentadol Surgery |
- Cold packs can be used in the acute inflammation phase
- hot packs can be used in the chronic muscle spasm phase
- Massage can improve pain, depression and sleep in the medium term
- activity modification be done in phases.
- A period of light activity and avoidance of painful activities is appropriate for several days.
- bed rest is not recommended
- early return to low-stress aerobic activity
- Physiotherapy-directed
- strengthening and posture control can start after the acute period and continue indefinitely.
- Core exercises are more effective than general exercise for decreasing pain and increasing function
- weight reduction
- loss of ≥5% body weight reducing the prevalence of LBP
- Multidisciplinary rehabilitation
- psychological therapy
- cognitive behaviour therapy
- progressive relaxation
- physical therapy
- occupational therapy
- social work
- Acupuncture
- found acupuncture superior to placebo in the short term
- Chiropractic interventions
- do not appear to be beneficial for chronic LBP when compared with standard treatment
- found a small benefit for spinal manipulation when compared with placebo, but it is not superior to conventional treatment.
- Given the rare but catastrophic risk from disc herniation leading to cauda equina syndrome (1:1 million), caution should be exercised before recommending spinal manipulation.
- psychological therapy
Pharmacological
- Paracetamol
- does not appear to be beneficial for patient with acute LBP when used in isolation
- NSAIDs
- Cochrane review showed that NSAIDs are more effective than placebo for reducing pain and disability without increased adverse events.
- While there is no difference in efficacy between NSAIDs, COX-2 inhibitors are effective and have fewer side effects when compared with traditional NSAIDs
- muscle relaxants
- antidepressants
- can be used in cases of chronic LBP
- TCA appear to work better than SSRI
- Muscle relaxants
- BaclofenBenzodiazepineCyclobenzaprine
- Appear to be more effective than placebo in reducing acute symptoms.
- When used in conjunction with NSAIDs, there is an additive effect.
- consider a short course of low-dose diazepam to be reasonable in patients with acute LBP and back spasm. – side effects, including drug abuse, dependence and drowsiness, preclude long-term use or higher doses.
- Corticosteroids have no advantage over placebo for the treatment of LBP without radiculopathy.
- Injection of local anaesthetic and corticosteroids may be useful for diagnostic and therapeutic purposes.
- Tramadol
- found mild improvement in short-term pain and function when compared with placebo
- Tapentadol
- centrally acting opiate agonist and noradrenaline reuptake inhibitor.
- is effective for treating musculoskeletal pain, such as chronic LBP.
- safe and efficacious in the treatment of chronic LBP.
- Opoids
- Only to be used sparingly and only for acute, difficult-to-control pain.
- adverse effects: drug misuse, dependency and variable efficacy.
- Patients who tolerated opiates had small short/intermediate-term improvements in pain. When opiates were compared with NSAIDs, no superior effect was identified