Back Pain Conditions
Mechanical low back pain
- Essentially well person, may be unilateral or bilateral, starts suddenly, may be recurrent
- Pain is generalised
- Worse later in the day
- Worse with movement
- Alleviated by rest/ and lying
- Exacerbated by sitting
- precipitated by an injury
Pathology:
- Spinal movement occurs at the disc and the posterior facet joints, and stability is normally achieved by a complex mechanism of spinal ligaments and muscles.
- Any of these structures may be a source of pain.
- An exact anatomical diagnosis is difficult, but some typical syndromes are recognized (see below).
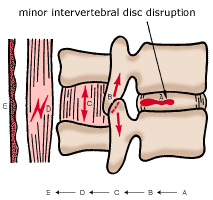
Reflex activity from a minor intervertebral derangement (MID) in the intervertebral motion segment.
- Apart from the local effect caused by the disruption of the disc (A),
- interference can occur in the
- facet joint (B)
- interspinous ligament (C) leading possibly to muscle spasm (D)
- and skin changes (E)
- Risk factors for recurrent back pain
- female sex
- increasing age
- pre-existing chronic widespread pain (fibromyalgia)
- psychosocial factors(distress, poor self-rated health, dissatisfaction with employment)
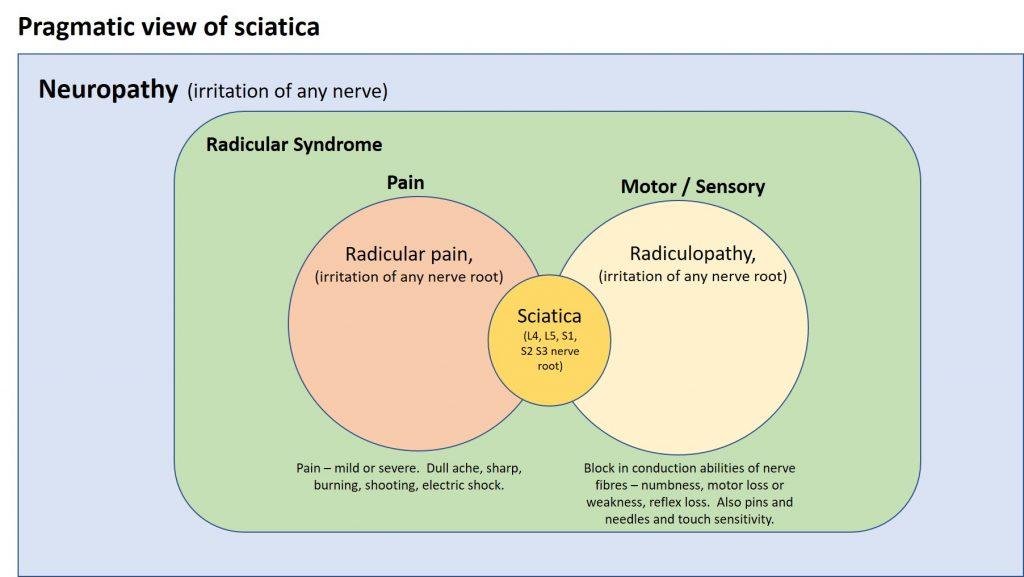
Lumbar radicular pain
- commonly referred to as ‘sciatica’, the term lumbar radicular pain (LRP) is anatomically more correct.
- Radicular pain:
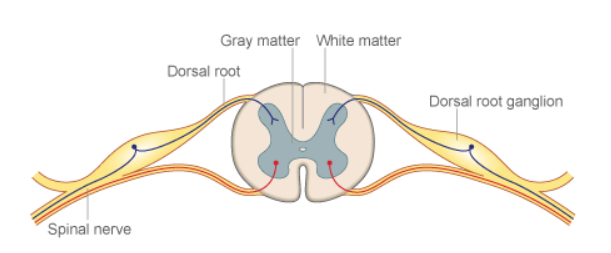
- pain that radiates into the lower extremity directly along the course of a spinal nerve root
- due to an irritation of the sensory root or the dorsal root ganglion (DRG) of a spinal nerve
- typically unilateral and follows a dermatomal pattern
- can be exacerbated by certain activities or maneuvers that put stress on the involved nerve root
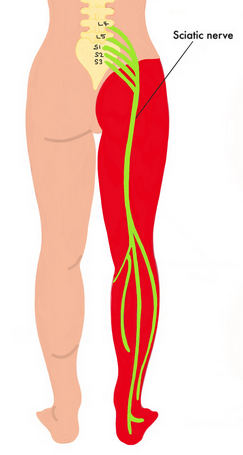
- Sciatic neuralgia
- pain in the distribution of the sciatic nerve due to pathology of the nerve itself ( causes: muscle spasm, bulging disc, inflamed joint)
Radicular pain should not be confused with radiculopathy
- Radiculopathy
- is objective loss of sensory and/or motor function as a result of conduction block
- the features of which might include
- numbness
- motor loss
- wasting
- weakness
- loss of reflexes.
- Each can occur simultaneously or independent of each other.
- Any lesion that affects the integrity of the lumbosacral nerve root can cause LRP, radiculopathy or both
- Causes of radicular pain
- Disc herniation (commonest cause)
- Spinal stenosis
- Synovial cysts
- Infection
- Infestation
- Tumour
- Vascular abnormalities
- Conditions mimicking radicular pain
- Spinal cord tumours
- Diabetic neuropathy
- The prodromal phase of herpes zoster
- Tabes dorsalis
- Direct contusion of the sciatic nerve
- Polyarthritis nodosa
- Gluteal injections
- Prolonged sitting
- Penetrating wounds
- Methyl methacrylate neuropathy following hip replacement
- Distinguishing features of LRP and somatic referred pain
- Note: They can co-exist. Radicular pain may be superimposed on a background of somatic referred pain
| Feature | Radicular pain | Somatic referred pain |
| Distribution | Entire length of lower limb But below knee > above knee | Anywhere in lower limb But proximal > distal |
| Pattern | Narrow band | Wide area |
| Quality | Travelling Quasi segmental but not dermatomal Not distinguishable by segment | Relatively fixed in location Quasi segmental but not dermatomal Not distinguishable by segment Boundaries difficult to define |
| Depth | Shooting, lancinating, like an electric shock Deep as well as superficial | Dull, aching, like an expanding pressure Deep only, lacks any cutaneous quality |
Other types of pain
- Nociceptive/Somatic pain
- afferent neurons are activated by a noxious stimulus (chemical, mechanical, or thermal in nature)
- pain localised to the area of injury – with or without somatic referral.
- Clear, proportionate and mechanical pain.
- Clear aggravating and easing factors.
- Pain is usually intermittent and sharp with mechanical provocation.
- Pain may be dull or a constant throb at rest.
- Local signs of inflammation (redness, heat and swelling) are present.
- Nociceptive pain was associated with the
- absence of
- dysaesthesia (abnormal sensation)
- night pain
- sleep disturbances
- burning pain
- shooting pain
- electric-like pain
- absence of
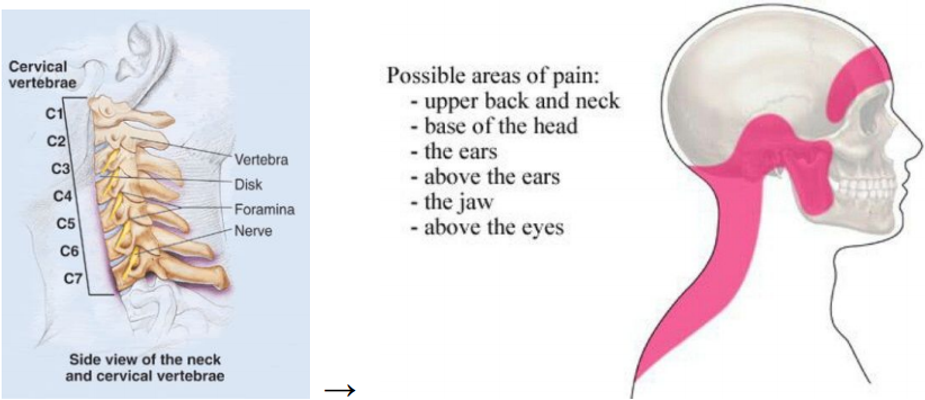
- Somatic referred pain
- This regards pain signals originating from somatic structures (such as joints, ligaments, muscles), which are interpreted by your brain as pain in another area of the body.
- Due to interneuronal convergence within the spinal cord.
- Pain-sensitive structures of the spine include the:
- Annulus fibrosus (outside layer) of the intervertebral disc
- Facet (zygapophyseal) joints
- Periosteum of the vertebrae
- Dura
- Epidural veins & arteries
- Ligaments
- Muscles


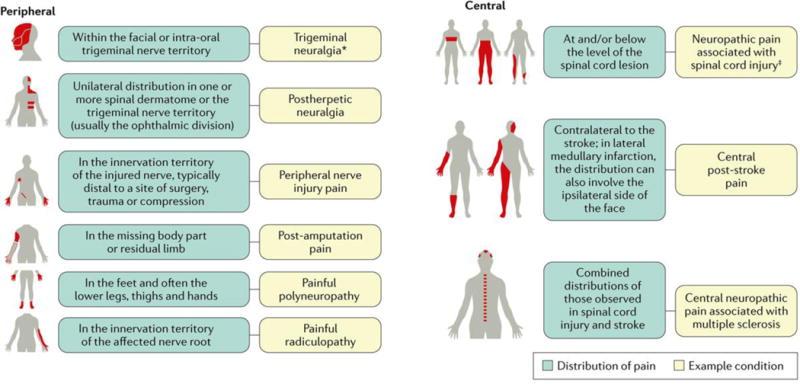
- Neuropathic pain
- pain caused by a lesion or disease of the somatosensory system.
- The somatosensory system allows for the perception of touch, pressure, pain, temperature, position, movement and vibration.
- The somatosensory nerves arise in the skin, muscles, joints and fascia and include thermoreceptors, mechanoreceptors, chemoreceptors, pruriceptors and nociceptors that send signals to the spinal cord and eventually to the brain for further processing
- most sensory processes involve a thalamic nucleus receiving a sensory signal that is then directed to the cerebral cortex.
- Lesions or diseases of the somatosensory nervous system can lead to altered and disordered transmission of sensory signals into the spinal cord and the brain
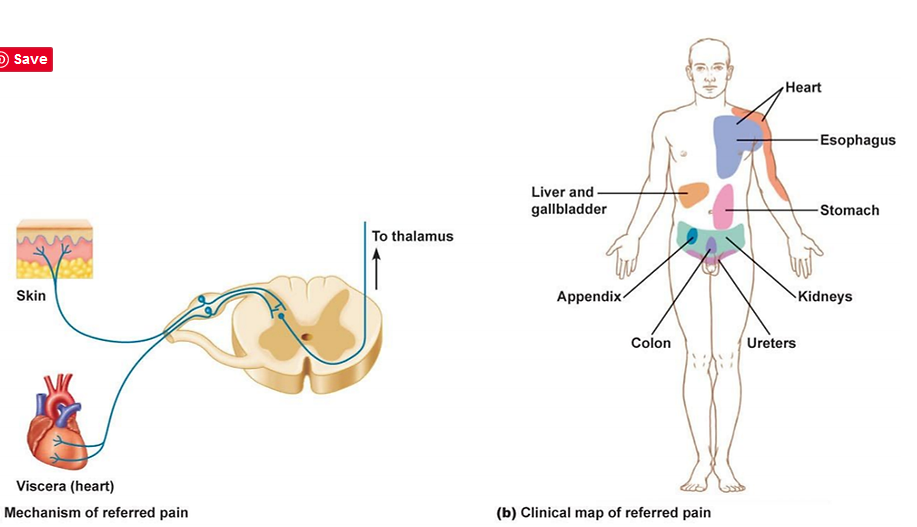
VISCERAL REFERRED PAIN:
Lumbar Spondylosis
- may be applied nonspecifically to any and all degenerative conditions affecting the disks, vertebral bodies, and/or associated joints of the lumbar spine
- Degenerative cycle includes
- disc degeneration: disc desiccation, loss of disc height, disc bulging, and possible disc herniation ⇒ spinal canal stenosis, subluxation of the facet joints
- joint degeneration: uncinate spurring and facet arthrosis, osteophytes form around the rim of the vertebra
- ligamentous changes: ligamentum flavum thickening and infolding secondary to loss of disc height
- deformity: kyphosis secondary to loss of disc height with resulting transfer of load to the facet and uncovertebral joints, leading to further uncinate spurring and facet arthrosis
- Associated conditions
- often leads to the clinical conditions of
- radiculopathy
- discogenic pain
- progressive spinal stiffening
- facet joint pain
- Facet joint syndrome
- acute disc prolapse, with or without nerve root irritation
- spondylolisthesis.
- often leads to the clinical conditions of
Scheuermann’s disorder

- Scheuermann disease, also known as juvenile kyphosis, juvenile discogenic disease, or vertebral epiphysitis, is a common condition which results in kyphosis of the thoracic or thoracolumbar spine.
- This condition is believed to be the result of a mismatch in the pubertal growth spurt, in which bone growth is not matched by increased bone strength.
- The diagnosis is usually made on plain radiograph.
- Epidemiology
- occurs in ~5% (range 0.4-8%) of the general population 2
- typical age of presentation is between 12 and 17 years 13
- slight male predominance
- Location
- Occurs in the thoracic spine in up to 75% of cases, followed by the thoracolumbar spine combined and occasionally lumbar and rarely cervical spine.
- The condition is associated with
- Schmorl nodes
- limbus vertebrae
- scoliosis (~25%)
- spondylolisthesis
- Treatment and prognosis
- Management is largely dependent on the degree of kyphosis:
- <50°: conservative, stretching, postural changes
- 50-75°: brace
- >75°: surgery
- Management is largely dependent on the degree of kyphosis:
Spondylolisthesis


- Spondylolisthesis is the slippage of one vertebral body with respect to the adjacent vertebral body causing mechanical or radicular symptoms or pain.
- It can be due to congenital, acquired, or idiopathic causes.
- pathology involves:
- A fractured pars interarticularis of the lumbar vertebrae, also called the isthmus.
- This affects the supporting structural integrity of the vertebrae, which could lead to slippage of the corpus of the vertebrae, called spondylolysthesis.
- In turn, leads to one of the most obvious manifestations of lumbar instability.
- Slippage can occur in 2 directions-
- anterior translation – anterolisthesis or
- backward translation – retrolisthesis
- neurologic symptoms caused by
- central and lateral recess stenosis
- a degenerative slip at L4/5 will affect the descending L5 nerve root in the lateral recess
- caused by slippage, hypertrophy of ligamentum flavum, and encroachment into the spinal canal of osteophytes from facet arthrosis
- a degenerative slip at L4/5 will affect the descending L5 nerve root in the lateral recess
- foraminal stenosis
- a degenerative slip at L4/5 will affect the L4 nerve root as it is compressed in the foramen vertical foraminal stenosis (loss of height of foramen) caused by
- central and lateral recess stenosis
- Etiology
- Repetitive stress to the pars interarticularis
- Decreased strength of the neural arch at a young age predisposes children and adolescents to a higher risk of fracture.
- Traumatic accidental injuries
- Microtrauma in sports
- Pathological causes – Neoplasm, connective tissue disease, etc.
- Iatrogenic – After laminectomy
- Adolescents and children also have more elastic intervertebral disks which cause increased stress to be placed on the pars interarticularis
- Symptoms
- mechanical/ back pain
- usually relieved with rest and sitting
- neurogenic claudication & leg pain
- second most common symptoms
- defined as buttock and leg pain/discomfort caused by upright walking
- relieved by sitting
- not relieved by standing in one place (as is vascular claudication)
- may be unilateral or bilateral
- same symptoms found with spinal stenosis
- cauda equina syndrome (very rare)
- mechanical/ back pain
- Physical exam
- L4 nerve root involvement (compressed in foramen with L4/5 DS)
- weakness to quadriceps
- weakness to ankle dorsiflexion (cross over with L5)
- decreased patellar reflex
- L5 nerve root involvement
- weakness to ankle dorsiflexion (cross over with L4)
- weakness to EHL (great toe extension)
- weakness to gluteus medius (hip abduction)
- provocative walking test
- have patient walk prolonged distance until onset of buttock and leg pain
- have patient stop but remain standing upright
- if pain resolves this is consistent with vascular claudication
- have patient sit
- if pain resolves this is consistent with neurogenic claudication (DS)
- have patient stop but remain standing upright
- hamstring tightness
- commonly found in this patients, and must differentiate this from neurogenic leg pain
- have patient walk prolonged distance until onset of buttock and leg pain
- L4 nerve root involvement (compressed in foramen with L4/5 DS)
- Radiographs
- Xray: slip is evident on lateral x-ray
- MRI -if persistent leg pain that has failed nonoperative modalities
- Treatment
- most patients can be treated nonoperatively
- NSAIDS
- Physiotherapy
- relieving extension stresses from the lumbosacral junction (hamstring and hip flexor stretching)
- working on core strengthening (deep abdominal muscles and lumbar multifidus strengthening).
- epidural steroid injections
- second line of treatment if non-invasive methods fail
- Operative
- Approximately 10% to 15% of younger patients with low-grade spondylolisthesis will fail conservative treatment and need surgical treatment.
- lumbar decompression with instrumented fusion, +/- interbody fusion
- decompressive surgery and Discectomy for herniated lumbar disc
- most patients can be treated nonoperatively
Surgery Indications
- Urgent and Emergent
- Cauda Equina Syndrome (emergent surgery)
- Progressive Motor Weakness (urgent surgical evaluation)
- Spinal Infection (e.g. Diskitis, Spinal Osteomyelitis, Spinal Epidural Abscess)
- Unstable Lumbar Vertebral Fracture
- Spinal Malignancy
- Other (poor surgical efficacy)
- Disabling Low Back Pain impacting quality of life for >1 year and refractory to conservative measures
- Common surgical procedures
- Spinal Fusion : Intervertebral discs resected and two or more Vertebrae are fused via bone grafts or metal bars
- Lumbar Disc Replacement
- Diskectomy : Removal of Herniated disc through a back incision (smaller incision in microdiskectomy)
- Spinal Laminectomy and Spinal decompression : Removal of the lamina (Vertebral bony walls) and bone spurs, Often performed in combination with Diskectomy, Performed to relieve pain, numbness or weakness due to nerve compression from a disc or bone spur
- Failed Back Surgery Syndrome (Postsurgical Spine Syndrome)
- Persistent Low Back Pain, radicular pain or weakness following surgical intervention
- Among the most common causes of Chronic Pain
- Associated with functional Disability, as well as psychosocial and unemployment impacts
Cauda Equina Syndrome
- Massive Central DIsc protrusion 🡪 Compression of lumbar spinal nerve roots
- Delayed diagnosis or misdiagnosis is not uncommon (even by neurosurgical senior residents)
- Anatomy
- The spinal cord terminates in the conus medullaris at the T12/L1 vertebral body in adults
- Cauda equina
- Collection of nerve roots from L1-S5
- Compression from various causes results in lower motor neuron pathology
- Causes
- Large Central DIsc Herniation
- Lumbar Spinal Stenosis
- Lumbar Spine Trauma
- Spinal Neoplasm
- Lumbar Spondylosis with cauda equina compression
- Epidural Hematoma
- Epidural Abscess
- Symptoms
- Bilateral Sciatica
- Dull aching pain in perineum, Bladder or Sacrum
- Radiation to Buttock and leg
- Provoked by Exercise or prolonged standing
- Relieved with rest or forward bending
- Neurologic Changes
- Saddle Anesthesia
- Bowel dysfunction (constipation and/or incontinence)
- Bladder Incontinence or Acute Urinary Retention
- Bilateral Sciatica
- Signs
- Loss of perineal Sensation or perineal reflex
- May best correlate with cauda equina findings on MRI
- Loss of rectal tone
- Increased post-void residual Urine Volume
- Foot Drop
- Ankle dorsiflexion bilateral weakness
- Absent Ankle Jerk
- Hypotonia/atrophy of the lower extremities (in chronic presentations)
- High yield exam findings
- Altered perineal Sensation
- Abnormal rectal tone
- Increased post-void residual
- Loss of perineal Sensation or perineal reflex
- Management
- Surgical decompression within 24 hours seems to have the best outcome
- Patients with complete cauda equina syndrome have a poorer outcome
- Approximately 20% of patients will have a poor outcome in terms of urological and/or sexual function, as well as lower limb paresthesia and weakness
Diffuse idiopathic skeletal hyperostosis (DISH)

- affects the spine and extraspinal locations.
- causes bony overgrowths and ligamentous ossification and is characterized by flowing calcification over the anterolateral aspects of the vertebrae.
- overall incidence 6-12%
- uncommon before 50 years old
- > 50 y.o. (25% males; 15% females)
- > 80 y.o. (28% males; 26% females)
- Location: occurs anywhere in spine
- The spine is stiff but not always painful – often asymptomatic and discovered incidentally
- XRAY: ‘whiskering’ due to ossification at muscle insertions around the pelvis
- A CT scan should be performed whenever there is concern for a fracture following low energy trauma.
- Treatment is usually activity modification, physical therapy, and bisphosphonate therapy. Associated spine fractures are treated with long spinal fusion.
- uncommon before 50 years old
Osteoporotic crush fracture of the spine
- vertebral fractures develop without trauma, after minimal trauma, or as part of a major accident
- pain: painlessly or agonizing localized pain that radiates around the ribs and abdomen.
- Multiple fractures lead to an increased thoracic kyphosis (‘widow’s stoop’).
- Xray: loss of anterior vertebral body height and wedging, with sparing of the vertebral end-plates and pedicles
- Non-Surgical Management
- Conservative Treatment: This includes bed rest, pain medication (like analgesics), physiotherapy, and bracing. Conservative management is usually the first line of treatment for patients with osteoporotic VCFs.
- Physical Therapy: Tailored exercises can help improve mobility and strengthen the muscles supporting the spine.
- Bracing: Orthotic devices can help stabilize the spine, reduce pain, and prevent further collapse of the fractured vertebra.
- Pain Management: Medications for pain control are crucial and may include over-the-counter or prescription pain relievers.
- Surgical Management
- Vertebroplasty and Kyphoplasty: These are minimally invasive procedures where bone cement is injected into the fractured vertebra to stabilize it. Kyphoplasty involves the use of a balloon to create space for the cement.
- Spinal Fusion: In severe cases where there is significant spinal instability or deformity, surgical fusion of the affected vertebrae may be necessary.
- Other Considerations
- Treatment of Underlying Osteoporosis: Alongside the direct management of the fracture, it’s crucial to treat the underlying osteoporosis to prevent future fractures. This may include medications like
- bisphosphonates
- calcium and vitamin D supplements
- lifestyle modifications.
- Treatment of Underlying Osteoporosis: Alongside the direct management of the fracture, it’s crucial to treat the underlying osteoporosis to prevent future fractures. This may include medications like