Developmental dysplasia of hip
– How to Treat article “ A GP guide to paediatric orthopaedics” Dec 2019, SCHP notes
= spectrum of conditions where the femoral head has abnormal relationship to acetabulum 🡪 unstable hip
- Associated with DS, neuromuscular conditions eg. Spina bifida, CP
- Physiological laxity of hip in newborns usually resolves after several weeks with normal development of acetabulum
Diagnosis
Clinical examination
- Hip instability demonstrated with Orotlani maneuver or Barlow maneuver
- Asymmetry of gluteal creases
- Asymmetry of limb length, particularly if >3/12 age
- ↓ hip abduction, partic if >3/12 age
- Positive Trendelenburg pelvic tilt test & lurch (if walking)
Other: Neuro (movement of all limbs, spasticity, ROM, foot abnormality)
- Physical exam (> 3 months to 1 year)
- limitations in hip abduction
- most sensitive test once contractures have begun to occur
- occurs as laxity resolves and stiffness begins to occur
- decreased symmetrically in bilateral dislocations
- leg length discrepancy predominates
- limitations in hip abduction
- Physical exam (> 1 year – walking child)
- pelvic obliquity
- lumbar lordosis: in response to hip contractures resulting from bilateral dislocations in a child of walking age
- Trendelenburg gait
- results from abductor insufficiency
- toe-walking
- attempt to compensate for the relative shortening of the affected side
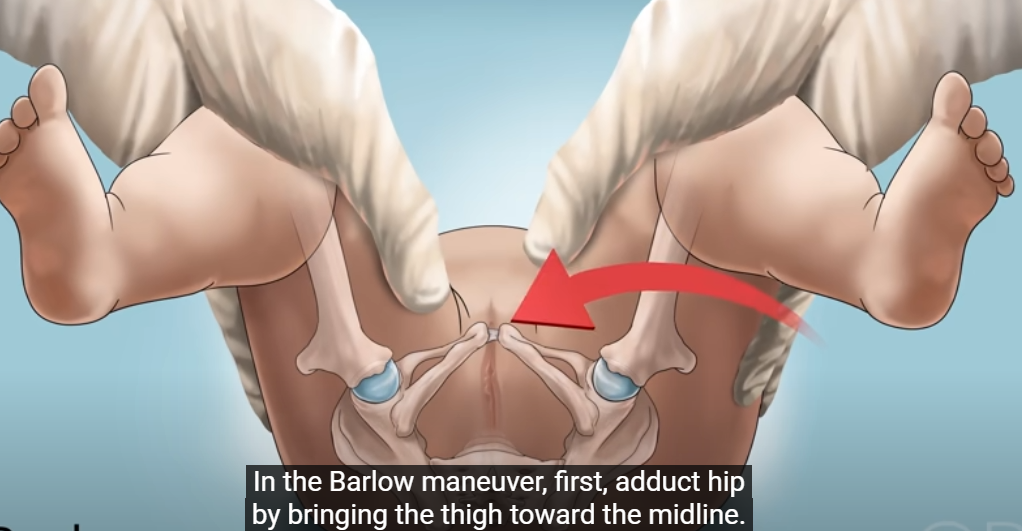
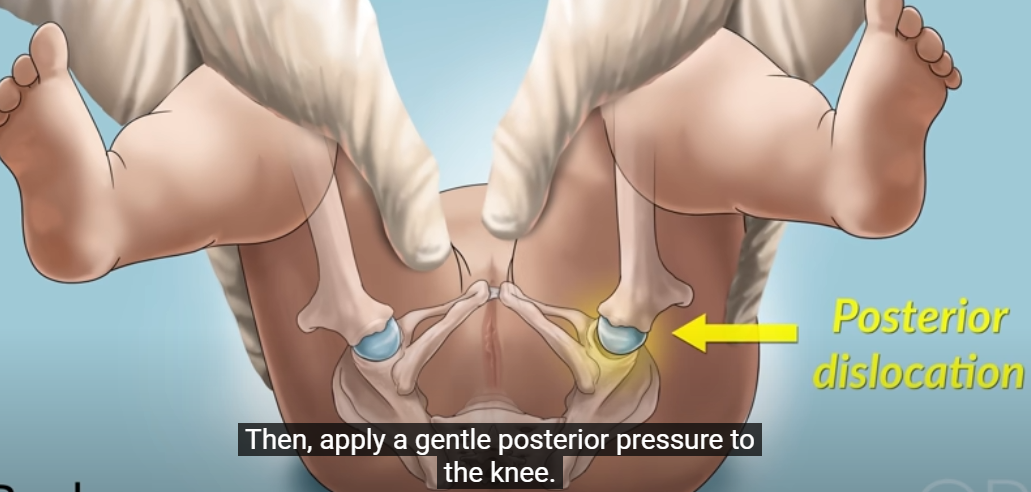
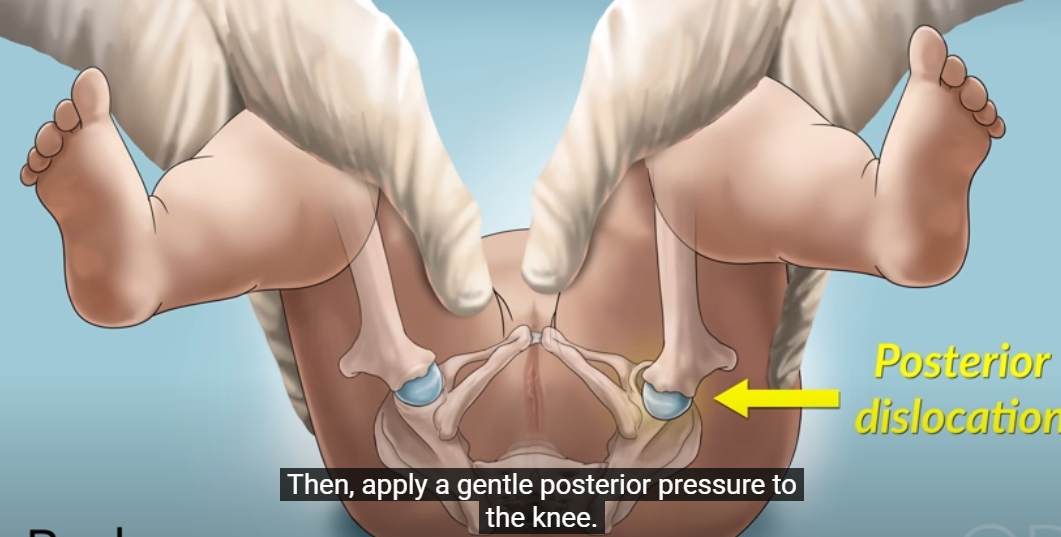
- Barlows Manoevre
- try and dislocate the flexed hip with a postero-lateral movement of the proximal femur = ‘click of exit’
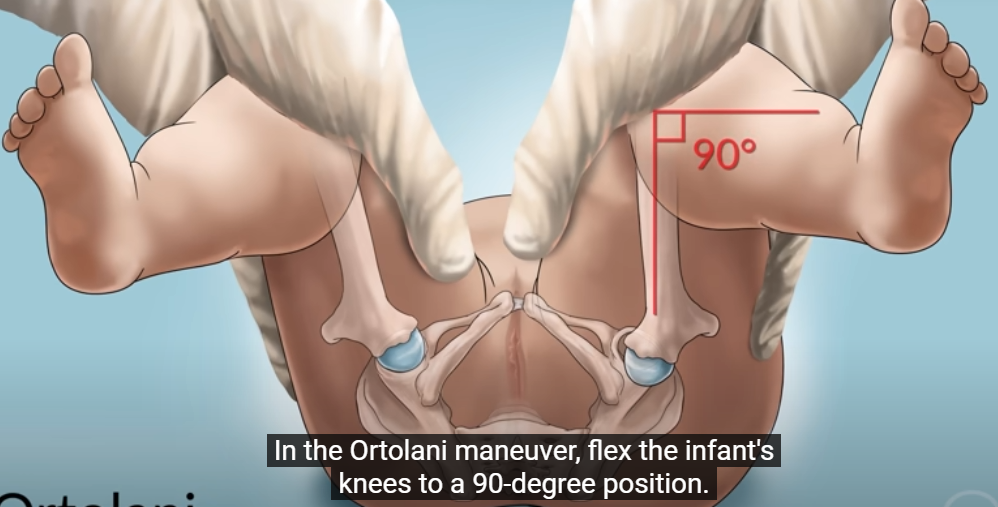
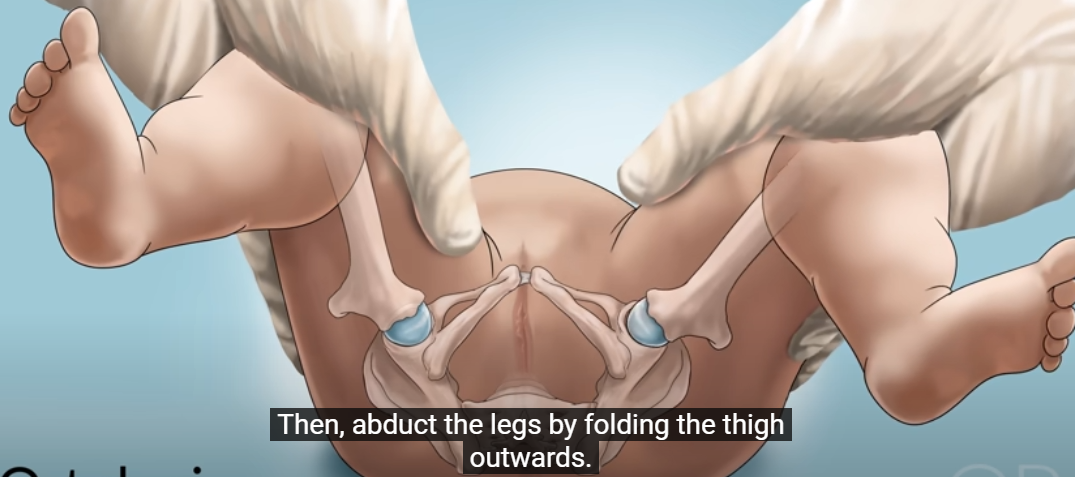
- Ortolani
- Then to feel the movement of the reduction of the dislocated hip back into the acetabulum by moving the femoral head anteriorly whilst the hip is abducted =’click of entry’

Risk factors:
- Female
- Breech position after K34
- Very tight swaddling of lower extremity
- Oligohydramnios
- intrauterine packaging deformities
- plagiocephaly
- foot deformities
- torticollis
- family history of DDH
Other: underlying NM dysfunction
Investigations
USS if < 4-6/12 age
- predominantly cartilaginous nature of the bones make x-rays an unsuitable means of assessing structure
- All babies with any of RFs or with abnormal hip examination should undergo a hip USS and review by paediatrician/ ortho surgeon
XRay if > 6/12 age
Management
- Non-operative
- abduction splinting/bracing (Pavlik harness)
- if < 6 months old and reducible hip. contraindicated in teratologic hip dislocations and patients with spina bifida or spasticity
- closed reduction and spica casting
- 6-18 months old and if failure of Pavlik treatment
- abduction splinting/bracing (Pavlik harness)
- Operative
- open reduction and spica casting if >18 months old, open reduction and femoral osteotomy
Possible sequelae (if left untreated)
- Disability
- Pain
- OA
- Disturbed gait
- Leg length discrepancy
- Other: Ipsilateral knee problems, scoliosis, back pain