elbow pain
causes of lateral elbow pain include:
- tennis elbow
- radial tunnel syndrome
- Medial elbow pain
causes of medial elbow pain include:
- golfer’s elbow
- cubital tunnel syndrome
- medial (ulnar) collateral ligament injury
Golfers elbow
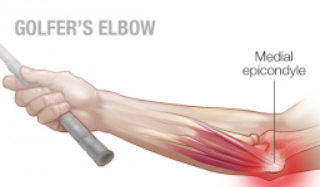
- Golfer’s elbow is caused by inflammation of the flexor rigin at the medial humeral epicondyle, where there is pain and tenderness. It is far less common than its counterpart tennis elbow.
- It is characterised by pain radiating across the flexor aspect of the arm and there is pain on resisted pronation.
- Medial epicondylitis is an overuse injury affecting the flexor-pronator muscles (i.e. pronator teres, flexor carpi radialis, palmaris longus) at their origin on the anterior medial epicondyle of the humerus
- onset can be related to occupation (e.g. consistent use of a tool such as a hammer, or in baseball when throwing a pitch)
- examination
- should reveal point tenderness of the medial aspect of the elbow over the common flexor origin
- this point can be found by palpating the elbow with the wrist held in resisted palmar flexion
- discomfort with this manoeuvre is confirmatory
- neurological examination of the upper limb should be normal
- joint is not involved so ROM should not be affected
- Investigation: diagnosis is made clinically
- ultrasound is the investigation of choice if there is any doubt over the diagnosis
- a nerve conduction study can be useful in excluding cubital tunnel syndrome
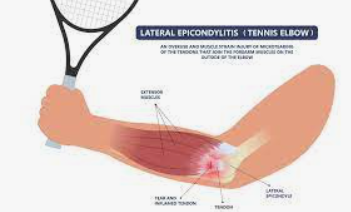
Tennis Elbow
- partially reversible but degenerative overuse-underuse tendinopathy
- Risk factors
- occupational activities and sports which involves repetitive wrist motion or a power grip
- some examples are plumbing; playing a musical instrument; painting; weaving; raking; using screwdrivers, pliers, and hammers; fishing; engaging in arm wrestling, racket sports, and other twisting movements; and lifting objects with an extended wrist
- Although the condition is named as tennis elbow, tennis is a direct cause in only 5% of people with lateral epicondylitis.
- More typically the condition occurs due to overuse of a previously underused and atrophied tendon.
- This is specially seen in people who begin exercising at the gym, start doing some gardening, painting a room, lifting a new baby, or even just carry heavy luggage on holiday after living a sedentary life style for years
- occupational activities and sports which involves repetitive wrist motion or a power grip
- symptoms
- gradual, insidious onset pain localized to the front of the lateral epicondyle and often radiates down the forearm
- pain is made worse by movements such as pouring out tea, shaking hands or lifting the wrist whilst the forearm is pronated.
- weakness in grip strength or difficulty in carrying objects in hands (2)
- examination
- there is no swelling
- the elbow can be flexed and extended without pain
- tenderness is generally localized to the lateral epicondyle over the extensor mass
- symptoms are usually reproduced with resisted supination or wrist dorsiflexion, particularly with the arm in full extension
- grip strength may be decreased (compared to the unaffected side) or may cause significant discomfort
- Treatment
- self limiting condition
- Non operative procedures:
- rest, application of ice
- NSAID’s
- physical therapy
- stretching and strengthening exercise – specially eccentric (lengthening only) exercises
- corticosteroid injections
- repeating and repeated corticosteroid injections has been reported that repeated injections (average 4.3, range 3 to 6 over 18 months) were associated with poorer outcomes – the suggestion is that steroid injections are more effective in acute and subacute tendonitis (duration <12 weeks
- orthotic devices
- extracorporeal shock wave therapy (ESWT)
- Surgery
- autologous platelet-rich plasma injections
- recent high quality randomised controlled trials have shown superior cure rates and pain scores for platelet-rich-plasma (PRP) injections up to two years after treatment when compared to cortisone injections
- botulinum toxin A injection
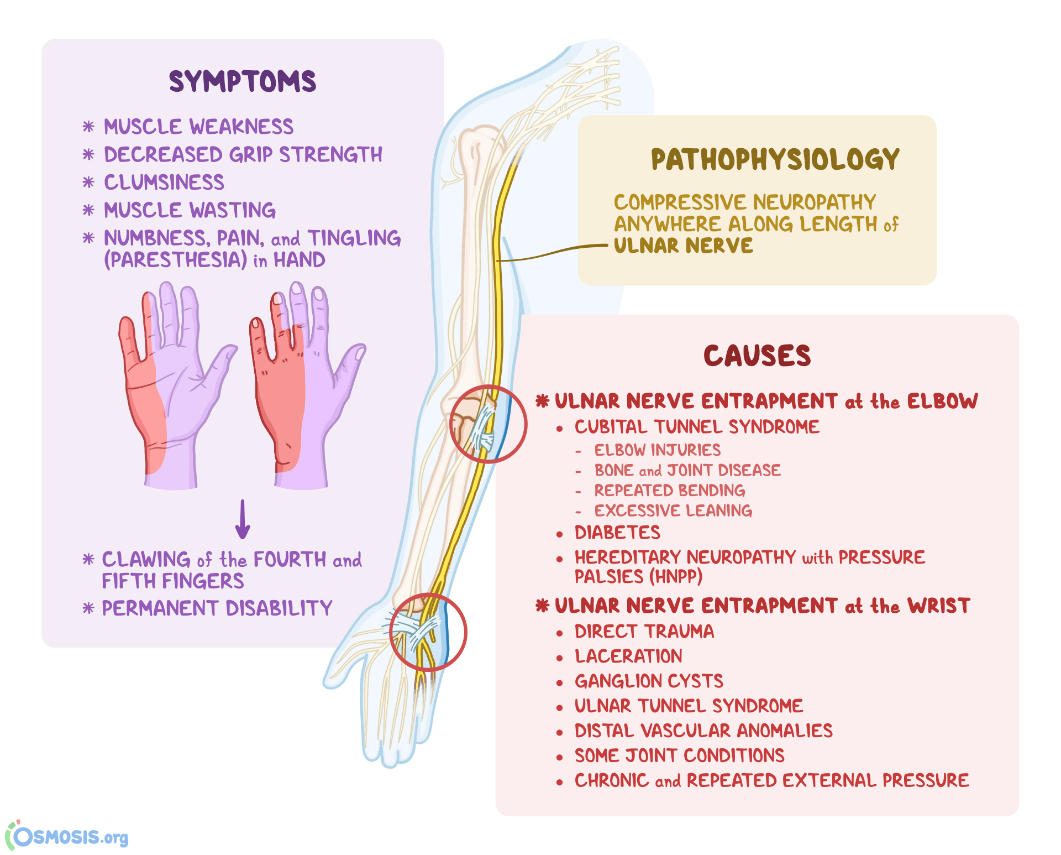
Cubital tunnel syndrome

- Entrapment of the ulnar nerve within the cubital tunnel and subsequent inflammation may present with medial elbow pain, hand weakness
- Patient c/o of pins and needles radiating down the medial forearm
- Examination
- positive Tinel’s test (medial elbow pain and 4th and 5th digit pins and needles upon tapping the cubital tunnel over the medial aspect of the elbow (‘funny bone’))
- positive Froment’s
- positive Wartenberg’s signs

- Investigation
- nerve conduction study
- a plain x-ray will show if there is bony impingement of the cubital tunnel
- ultrasound may show swelling of the ulnar nerve and is useful in confirming the position of the ulnar nerve before surgery
- Management
- patients with mild sensory symptoms may benefit from ergonomic advice and physiotherapy
- ultrasound-guided injections of hydrocortisone may offer temporary relief
- patients presenting with weakness (positive Froment’s and Wartenberg’s) should be referred for surgical decompression