FOOT AND ANKLE
March fractures
- fatigue/stress fractures
- occur due to repeated concentrated trauma to a normal bone
- classically the 2nd metatarsal of the foot but can occur in other weight-bearing bones of the lower limb and pelvis

- Imaging
- Radiographs
- AP, lateral and oblique views of the foot
- CT
- not routinely obtained
- may be of use in periarticular injuries or to rule out Lisfranc injury
- MRI or bone scan
- useful in detection of occult or stress fractures
- Radiographs
- Treatment
- Nonoperative
- stiff soled shoe or walking boot with weight bearing as tolerated
- if non-displaced fractures – second through fourth (central) metatarsals
- isolated fractures – non-displaced or minimally displaced fractures
- stress fractures – second metatarsal most common
- stiff soled shoe or walking boot with weight bearing as tolerated
- Nonoperative
Sever’s Disease
- caused by overuse injury of the calcaneal apophysis
- frequently seen just before or during peak growth
- presents in children 7-15yo (usually boys)
- Painful tender heel at insertion, diagnosed by XR


- Symptoms
- presents with posterior heel pain
- pain in the area of the calcaneal apophysis in an immature athlete
- pain increased with activity or impact
- stretch of the triceps surae exacerbates heel pain
- can display warmth, erythema, & swelling
- Physical exam
- tight Achilles tendon
- positive squeeze test (pain with medial-lateral compression over the tuberosity of the calcaneus)
- pain over the calcaneal apophysis
- Diagnosis
- made clinically with tenderness over the calcaneal apophysis
- foot radiographs:
- sclerosis and fragmentation of the calcaneal apophysis
- MRI
- can help localize inflammation to apophysis
- can rule out disorders of the body of the os calcis (stress fracture, lytic lesion, osteomyelitis)
- Treatment
- activity modifications
- heel cups or heel pads
- avoid flat-heeled shoes
- slightly raised heel
- restrict strenuous sport for 3 months
- Achilles tendon stretches
Cracked heels
- Predisposition may be due to:
- Dry skin
- Atopic dermatitis
- Juvenile plantar dermatosis
- Psoriasis, especially palmoplantar psoriasis
- Palmoplantar keratoderma
- Systemic conditions, including diabetes and hypothyroidism
- Dry thickened skin (corn and callus) around the rim of the heel is the very first step towards cracking.
- Increased pressure on the fat pad under the heel causes it to expand sideways, leading to splitting or cracking of the callus.
- Some factors that contribute to cracking or splitting include:
- Excessive weight or obesity
- Prolonged standing, especially on hard floors
- Open-back shoes and sandals, as they provide no support to hold the fat pad under the foot
- treatment
- The best form of treatment for cracked heel is to prevent cracks from occurring in the first place.
- moisturising cream on a regular basis to keep the skin supple and hydrated.
- Special heel balms are available that contain descaling (keratolytic) or water-retaining (humectant) agents, such as:
- Urea
- Salicylic acid
- Alpha-hydroxy acids
- Saccharide isomerate
- Debridement – cutting away hard thick skin (this should not be attempted at home using scissors or razor blade as there is a risk of removing too much skin and infection occurring)
- Strapping – bandage/dressings around the heel to reduce skin movement
- Prescription for stronger softening or debriding agents, usually containing urea or salicylic acid
- Insoles, heel pad or heel cups to redistribute the weight of the heel and provide better support (prevent the fat pad from expanding sideways)
- Hydrocort 0.5% if resistant
- For severe cases use sorbolene cream with 20% glycerol and 30% urea (test skin sensitivity first)
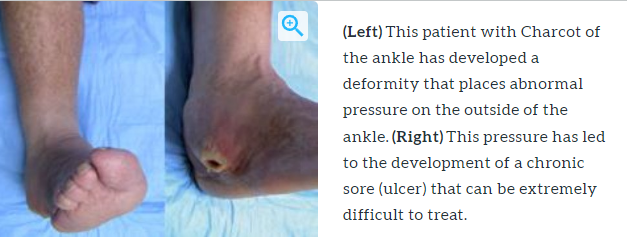
Charcot’s foot


- a neuroarthropathic process with osteoporosis, fracture, acute inflammation and disorganisation of foot architecture.
- During the acute phase, Charcot’s foot can be difficult to distinguish from infection.
- SSx: red, swollen oedematous and possibly painful foot in the absence of infection.
- It is associated with increased bone blood flow, osteopenia and fracture or dislocation
- Charcot arthropathy is a condition of the foot and ankle caused by an inability to sense injuries, which can result in significant deformities.
- Neuropathy (nerve damage) MUST be present for Charcot foot to develop, and the most common cause of that neuropathy is diabetes.
- Diabetic patients with neuropathy can sustain fractures or dislocations in the foot without realizing it.
- These injuries can:
- Occur from obvious traumatic events, such as falls or ankle sprains.
- Develop slowly over time as a result of altered weight distribution on a diabetic foot (microtrauma).
- In a normal patient, these atypical forces would generate pain, causing the patient to automatically adjust their stance and redistribute weight before any injury or damage occurs in the foot.
- A diabetic, however, will not sense pain or adjust their weight, so these forces can cause fractures and other injuries over time.
- Without normal pain sensation, a diabetic may continue to walk on an injured foot, worsening the injury and leading to significant deformity.
- Only about 25 to 50% of patients with Charcot foot report a specific injury that they can recall.
- other risk factors that can contribute to Charcot:
- obesity
- alcoholism
- leprosy
- myelomeningocele
- tabes dorsalis/syphilis
- syringomyelia
- The resulting deformities in Charcot foot can lead to several problems:
- They can make normal shoe wear difficult or even impossible.
- They can be significant enough to make the foot and ankle unstable and thus unable to support normal walking.
- The ultimate problem in Charcot, however, is that the deformities can create areas of prominent bone under the skin (the bone is immediately below the skin surface).
- This leads to ulcers, or wounds that are caused by excess pressure on the skin. Once the skin breaks, the risk of developing an infection in the foot is very high, and due to poor blood flow, diabetics have a difficult time both healing wounds and fighting infections.
- For this reason, diabetics with Charcot foot have a 50% chance of ending up with an amputation if they develop an ulcer, as opposed to only a 10% chance without an ulcer.

Management
- Nonoperative
- total contact casting
- mainstay treatment for focusing on offloading the foot to manage the condition
- casts changed every 2-4 weeks for 2-4 months
- shoewear modifications focusing on offloading the foot
- orthotics
- Charcot restraint orthotic walker (CROW) boot can be used after contact casting
- shoe modifications
- medications
- bisphosphonates
- neuropathic pain medications
- antidepressants
- topical anesthetics
- outcomes
- 75% success rate
- total contact casting
- Operative
- resection of bony prominences (exostectomy) and TAL
- deformity correction, arthrodesis +/- osteotomies
- amputations
- indications
- failed previous surgery (unstable arthrodesis)
- recurrent infection
- indications
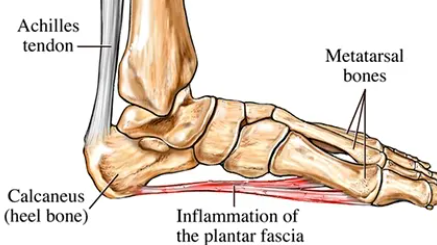
Plantar fasciitis
- inflammation of the plantar fascia aponeurosis at its origin on the calcaneus.
- Symptoms
- Pain on plantar aspect of heel, first steps out of bed
- relieved with walking
- worse after sitting
- worse at the end of the day after prolonged standing
- Pain on plantar aspect of heel, first steps out of bed
- exam
- tender to palpation at medial tuberosity of calcaneus
- dorsiflexion of the toes and foot increases tenderness with palpation
- limited ankle dorsiflexion due to a tight Achilles tendon
- tenderness at origin of abductor hallucis
- Imaging
- not necessary on initial visit and often normal
- Xray may show: may show plantar heel spur
- Bone scan – useful to rule out stress fracture
- Heals self in 12-24 months.
- Treatment
- Variable response to NSAID, injections, achilles/plantar fascia stretching, and orthotics
- non-pharmacological approach
- Stretching Exercises
- Physical Therapy
- Activity Modifications
- Footwear Modifications = use of runner’s shoes, crepe-soled shoes, or other supportive shoes, along with heel cushions or low-profile plastic heel cups,
- Rest and Ice: Resting the affected foot and applying ice can help reduce inflammation and alleviate pain
- Night Splints: The use of night splints, which keep the foot in a dorsiflexed position during sleep

Hallux rigidus
- OA of first MTP can lead to gradual loss of motion of toe and much discomfort
- Pain and stiffness
- in the big toe during use (walking, standing, bending, etc.)
- aggravated by cold, damp weather
- Difficulty with certain activities (running, squatting)
- Swelling and inflammation around the joint
- Rx
- Shockwave therapy
- NSAIDs
- Steroid injection
- Roomy footwear
- relative rest
- daily self-mobilisation
- Surgery for severe cases
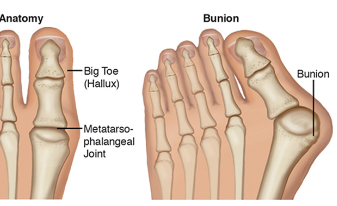
Hallux Valgus
- commonly referred to as a bunion
- can be a consequence of poor-fitting footwear
- Associated conditions
- hammer toe deformity
- callosities
- Pain might be due to shoe pressure, hammer toe, metatarsalgia or secondary arthritis
- Rx:
- Correct footwear
- surgical correction
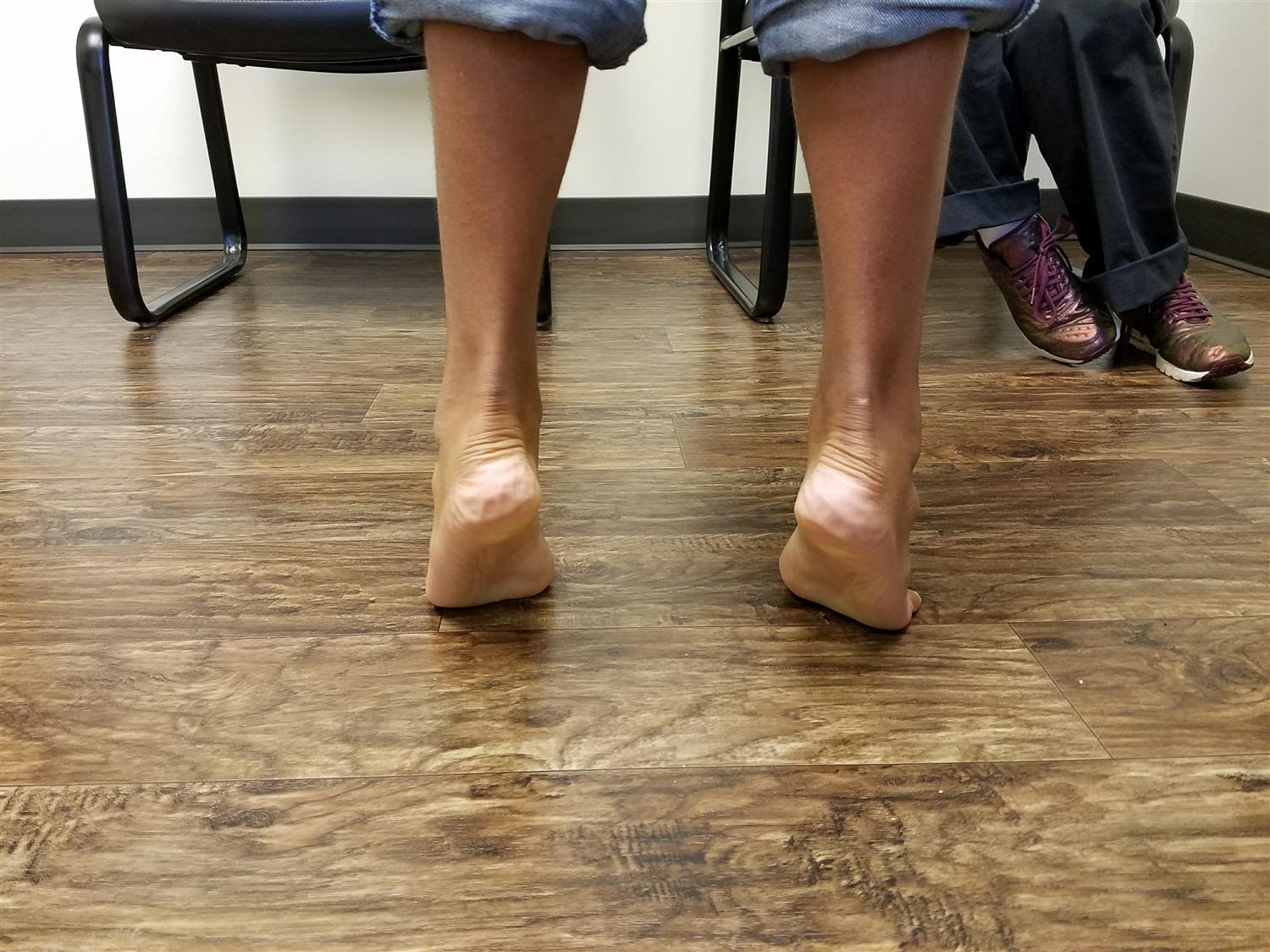
Pes planus (flat feet)
- Normal in young children
- foot arches usually develop with age
- no concern if arch restored by standing tiptoe.
- Incidence
- Flat feet are relatively common in childhood, affecting up to 14% of children.
- 20% to 25% in adults
- is common in children with Down syndrome
- Symptoms
- usually asymptomatic in children
- may have arch pain or pretibial pain
- Physical exam
- inspection
- motion
- normal and painless subtalar motion
- hindfoot valgus corrects to a varus position with toe standing
- evaluate for decreased dorsiflexion and tight heel cord
- The goal is not to reverse the changes but rather to help limit progression of the deformity and reduce the rate of chronic, secondary complications
- Non-Pharmacological
- Exercise therapy to strengthen foot muscles
- Shoe modifications, including medial longitudinal arch support and Thomas heel
- Use of orthotics to support the foot arch
- Physiotherapy and rehabilitation measures
- In severe cases, surgical interventions like arthroreisis of the sub-astragalic joint may be considered
- weight-bearing lateral foot radiograph

Pes cavus (claw foot)
- High foot arch, usually congential, could be due to polio or various neurological conditions
- Foot is inflexible, toes may be hammer or clawed. Special orthotics, good footwear, foot exercises, padding under MT heads

Osteochondritis/aseptic necrosis
- thought to be related to a disruption in the blood supply due to microtrauma or osteonecrosis and stress overloading
Kohler’s disorder
(Navicular)
- avascular necrosis of the navicular bone
- occurs in young children (usually age 4-7 yrs)
- four times more common in boys than girls
- 80% of cases in boys
- Painful limp, with some swelling and tenderness around navicular
- NSAIDS and immobilization with short leg walking cast
- Typically a self-limiting condition Intermittent symptoms for 1-3 years after diagnosis typically associated with activity

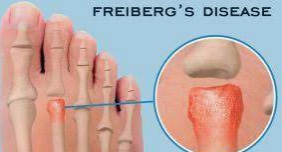
Freiberg’s disorder
- 🡪 head of second metatarsal
- disruption in the blood supply due to microtrauma or osteonecrosis and stress overloading
- leads to eventual collapse of 2nd MT head
- 12-16yo girls, forefoot pain, swelling and stiffness localized to head of the second MT worse with weight bearing activities
- Tender and swollen head of 2nd metatarsal on palpation,
- Plain XR – collapse of metatarsal head
- Restriction of activity, protective footwear, protective padding
- disruption in the blood supply due to microtrauma or osteonecrosis and stress overloading
Morton’s Neuroma
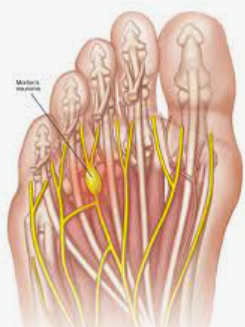
- Thickening/swelling of the nerve. Cause unknown. Clinical diagnosis
- Adults <50yo, commonest between 3rd and 4th MT heads, and between 2nd and 3rd MT heads
- Severe burning pain, worse on WB on hard surfaces, aggravated by tight shoes, relieved by squeezing
- Conservative initially, wearing loose shoes, low heel, sponge rubber MT pad. ORthrosis. Most eventually need excision
Sesamoiditis

- inflammation and swelling around the sesamoid (tibial > fibular) and FHB
- secondary to trauma, infection, AVN, stress fractures, Chondromalacia, OA or a systemic disorder;
- symptoms include pain on wt bearing and with dorsiflexion of the great toe and pain with direct palpation;
- Special sesamoid XR helps diagnosis.
- Mx: Well-designed insoles, surgical excision if persistent
Stress fractures
- Bone scan is only way to confirm suspected diagnosis. Common in dancers and the unfit restarting sport
- Absolute rest for at least 6 weeks with strong supportive footwear. Plaster not recommended
Ingrown Toenail
- Imbalance between soft tissues of the nail fold and the growing nail edge
- Exacerbated by faulty nail trimming and poor
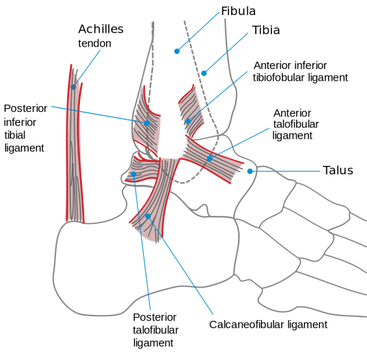
Sprained ankle
- most common ankle sprain is of the lateral or outside part of the ankle.
- There are three lateral ligaments
- Anterior Talofibular ligament (ATF)
- Calcaneofibular ligament (CF)
- Posterior talofibular ligament (PTF)
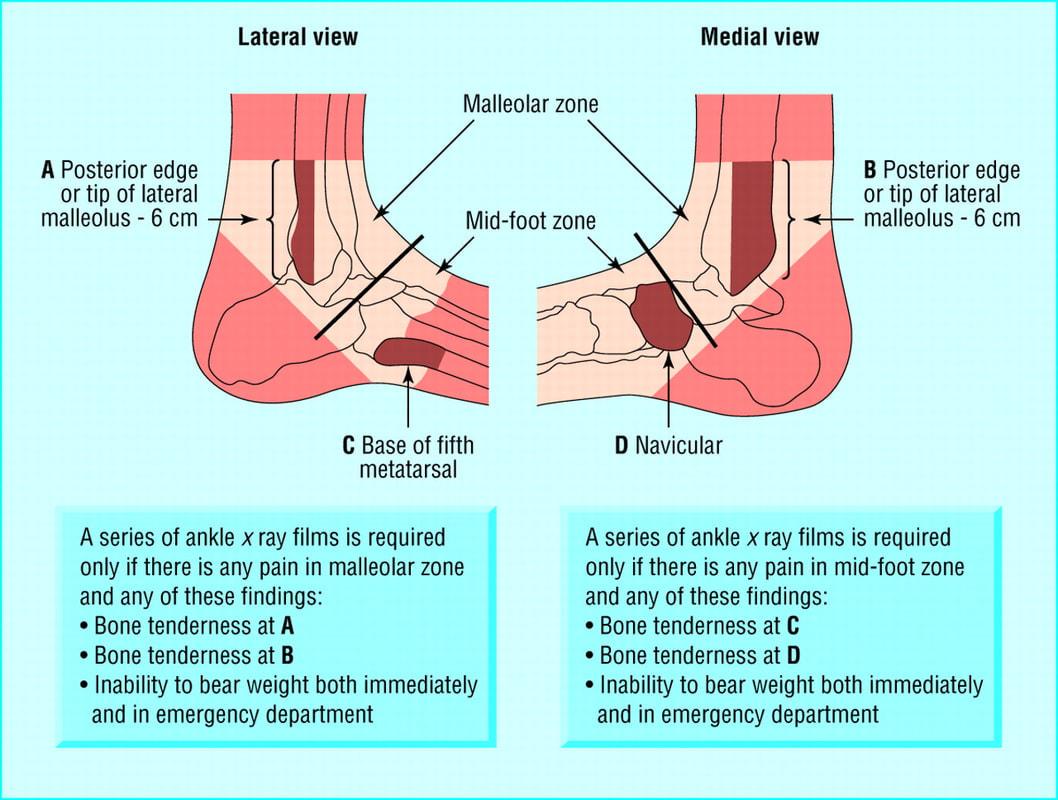
- Diagnosis can be made clinically with swelling and ecchymosis of the ankle and pain with range of motion.
- Radiographs are only indicated when clinical examination meets criteria (Ottawa ankle rules).
- Treatment usually includes a brief period of immobilization followed by early functional physical therapy.
- Rarely, operative management is indicated in the setting of syndesmosis injury with tibiofibular diastasis or chronic ankle instability with recurrent sprains.
Tarsal tunnel syndrome
- Tarsal tunnel syndrome is a compression, or squeezing, on the posterior tibial nerve that produces symptoms anywhere along the path of the nerve running from the inside of the ankle into the foot.
- Tarsal tunnel syndrome is similar to carpal tunnel syndrome, which occurs in the wrist. Both disorders arise from the compression of a nerve in a confined space.
- Causes of Tarsal Tunnel Syndrome
- An enlarged or abnormal structure that occupies space within the tunnel can compress the nerve.
- Some examples include a varicose vein, ganglion cyst, swollen tendon or arthritic bone spur.
- An injury, such as an ankle sprain, may produce inflammation and swelling in or near the tunnel, resulting in compression of the nerve.
- Systemic diseases, such as diabetes or arthritis, can cause swelling, thus compressing the nerve.
- An enlarged or abnormal structure that occupies space within the tunnel can compress the nerve.


- Symptoms of Tarsal Tunnel Syndrome
- Tingling, burning or a sensation similar to an electrical shock
- Numbness
- Pain, including shooting pain
- Symptoms are typically felt on the inside of the ankle and/or on the bottom of the foot.
- Nonsurgical Treatment
- Rest. Staying off the foot prevents further injury and encourages healing.
- Ice.
- Apply an ice pack to the affected area, placing a thin towel between the ice and the skin. Use ice for 20 minutes and then wait at least 40 minutes before icing again.
- Oral medications.
- Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation.
- Immobilization.
- Restricting movement of the foot by wearing a cast is sometimes necessary to enable the nerve and surrounding tissue to heal.
- Physical therapy.
- Ultrasound therapy, exercises and other physical therapy modalities may be prescribed to reduce symptoms.
- Injection therapy. Injections of a local anesthetic provide pain relief, and an injected corticosteroid may be useful in treating the inflammation.
- Orthotic devices.
- Custom shoe inserts may be prescribed to help maintain the arch and limit excessive motion that can cause compression of the nerve.
- Shoes. Supportive shoes may be recommended.
- Bracing.
- Patients with flatfoot or those with severe symptoms and nerve damage may be fitted with a brace to reduce the amount of pressure on the foot
Tarsal Coalition

- An abnormal connection of two or more tarsal bones in the foot.
- Commonly results in a severe, rigid flatfoot.
- Often present at birth but symptoms typically appear in early adolescence.
- Causes foot stiffness and pain, hindering everyday physical activities.
- Anatomy:
- Involves hindfoot and midfoot.
- Most commonly affects the calcaneus, talus, and navicular bones.
- Description:
- Coalition occurs when two bones grow together, connected by bone, cartilage, or fibrous tissue.
- Common sites: between the calcaneus and navicular bones, or between the talus and calcaneus bones.
- About 1 in 100 people may have a tarsal coalition, with 50% of cases affecting both feet.
- Begins before birth due to a gene mutation.
- Ossification typically happens between ages 8 and 16.
- Symptoms:
- Stiff, painful feet, especially below the ankle.
- Rigid, flat foot, difficulty walking on uneven surfaces.
- Increased pain or limp with high levels of activity.
- Diagnosis:
- CT scans – the gold standard for imaging tarsal coalitions
- Treatment:
- Nonsurgical: Rest, orthotics, temporary boots or casts, and steroid injections.
- Surgical: Resection (removing the coalition) or fusion (for severe cases with significant deformity or arthritis).
Achilles tendonitis

{kind=link}
{kind=link}
- consists of a series of 3 conditions affecting the achilles tendon which include:
- insertional Achilles tendonitis
- retrocalcaneal bursitis & Haglund deformity
- Achilles tendonitis.
- Diagnosis can be made with radiographs showing spurs and intratendinous calcification and in the case of Haglund deformity, an enlargement of the posterosuperior tuberosity of the calcaneus.
- Treatment is a trial of nonoperative management of NSAIDs, activity modification, shoe wear modifications, and physical therapy. Surgical management is indicated in patients with progressive symptoms who fail conservative management.
Achilles tendon rupture
- Most common tendon rupture in the lower extremity.
- Common in men between 30-40 during recreational sports.
- Presents with sudden pain and a “pop” sound at the injury site, leading to pain and disability.
- Often occurs in “weekend warrior” athletes involved in sporadic sports like soccer, basketball, or racket sports.
- 20-25% of cases are misdiagnosed as ankle sprains
- Etiology (Causes and Risk Factors):
- Causes: Sudden forced plantar flexion, direct trauma, long-standing tendinopathy.
- Risk factors:
- Poor conditioning before exercise
- corticosteroid use
- fluoroquinolone antibiotics
- oral bisphosphonates
- existing Achilles tendinopathy
- diabetes
- hyperparathyroidism, genetic factors.
- Clinical Presentation:
- Symptoms:
- Acute, sharp pain following a sport activity, difficulty in toe standing, or weakness in ankle plantar flexion
- Physical Exam:
- Thompson test to assess tendon continuity – squeezing the calf muscles of a prone patient should normally cause the foot to plantar flex. A negative test (no movement of the foot) indicates a rupture (Thermann, 2019).
- Symptoms:
- Treatment/Management:
- Nonoperative:
- Rest
- elevation
- pain control
- functional bracing.
- Operative: Various surgical techniques, including open repair, mini-open repair, and minimally invasive repair.
- Surgical repair aims to reapproximate torn tendon ends, with specific techniques chosen based on the injury.
- Nonoperative:
- High-level professional athletes often report inferior results and return to play regardless of the chosen management plan =>30% failure to return to play
- Differential Diagnosis:
- Includes conditions like Achilles bursitis, ankle fractures, DVT, gastrocnemius or soleus muscle strain, and others.
Lisfranc fracture
Tarsometatarsal fracture-dislocation
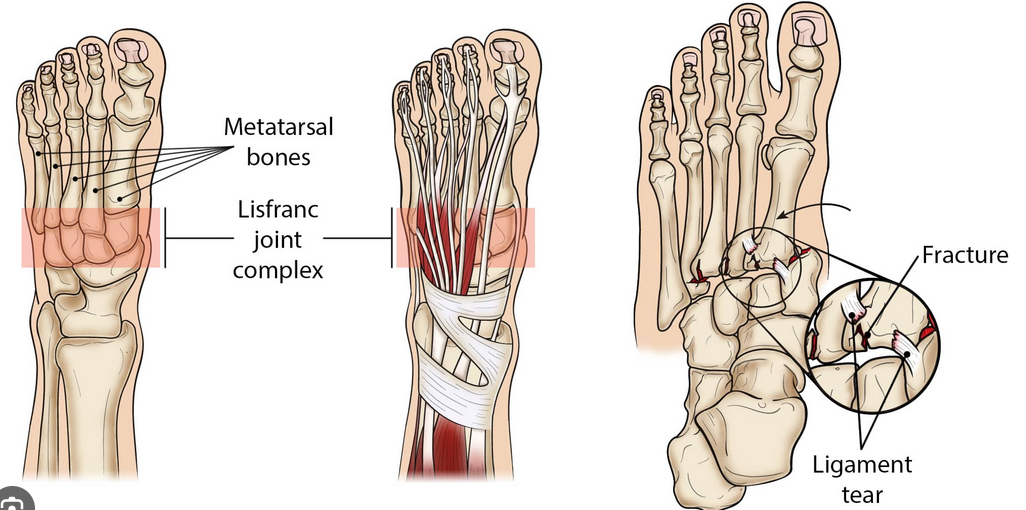

- A Lisfranc injury is a midfoot injury that results in displacement of one or more of the metatarsal bones from tarsus.
- history of high energy trauma or sporting accident
- Symptoms
- severe midfoot pain
- inability to bear weight
- XR
- widening of the space between the 1st and 2nd metatarsals
- Getting contralateral XR may help you identify this.
- Even if you don’t see that widening on the XR, the patient could still have a Lisfranc injury.
- If they cannot walk due to pain, get a weight bearing XR or CT scan to look further.
- Once the injury is identified, the patient must be strict non-weightbearing.
- Place them in a posterior splint and get orthopedics involved either in the ED or for prompt follow up as the patient will probably need surger