NECK PAIN
Epidemiology
- 15% of soft tissue problems seen in GP
- 1 year incidence of neck pain 10-20%; recurrence of 50%.
- F>M
Classification
- Acute < 6 weeks
- Subacute 6 weeks – 6 months
- Chronic > 6 months
Causes of Neck Pain
ASSESS FOR RED FLAG SYMPTOMS
- Mechanical
- Discogenic
- Myofascial
- Ligaments
- Spondylosis (degeneration)
- Fractures (eg in the setting of trauma)
- Neurological
- Myelopathy
- Cervical root compression
- Inflammatory
- Autoimmune spondyloarthropathies
- Rheumatological conditions
- Cardiovascular:
- Referred pain from cardiac ischaemia
- Carotid or vertebral artery dissection
- Infections
- Malignancies
Also assess for yellow flags (psychosocial factors).
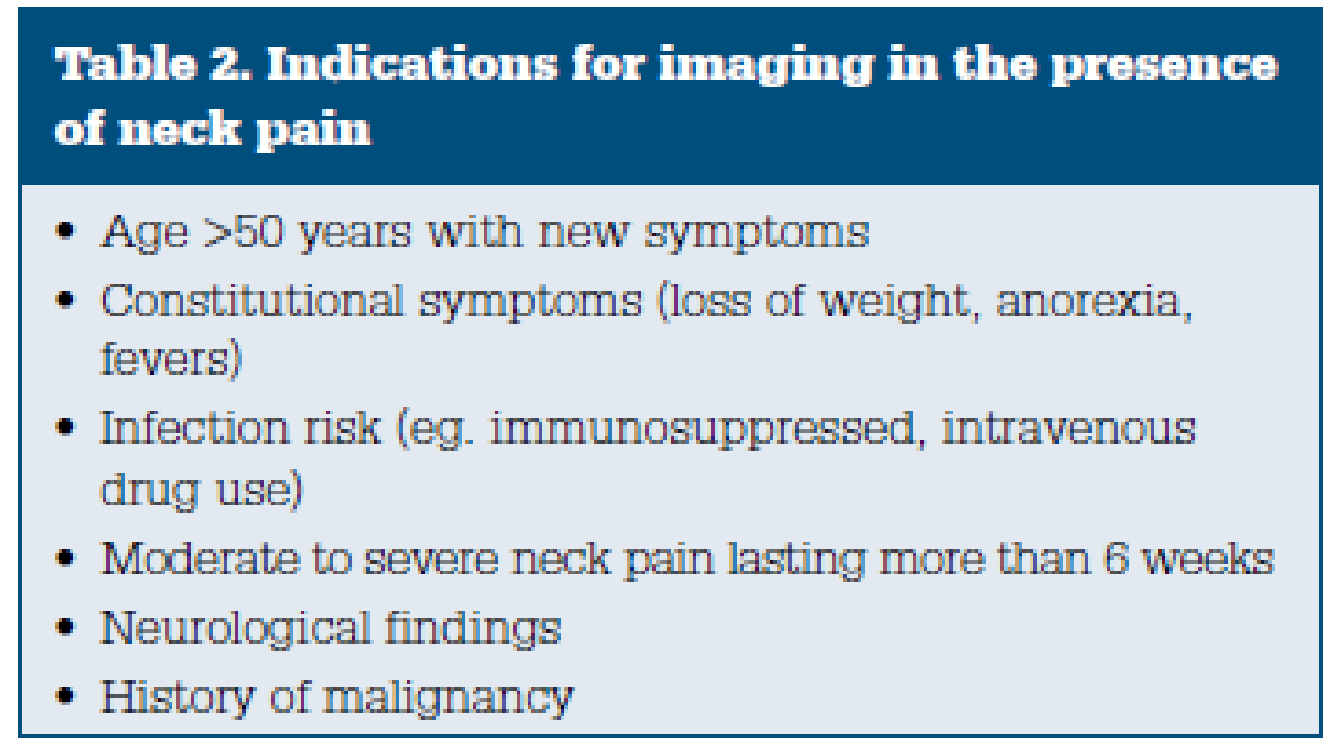
Imaging
Do not routinely refer for neck imaging unless there are concerns of red flags, or if the patient is having ongoing pain > 6 weeks.
Imaging choices:
- XR: first line
- CT: better for bone
- MRI: better for spinal cord, nerve roots, and soft tissue
Treatment
Non-pharmacological
- Exercise and physiotherapy leads to improvement of symptoms at 26 weeks, but not at 52 weeks.
- Acupuncture has short term benefits, but these are not sustained.
- Facet steroid injections – improvement in 40% of cases, but the procedure has significant risks.
- Address psychosocial factors.
Pharmacological
- Paracetamol and NSAIDs are first line
- Controlled release opioid have been shown to be efficacious but has its own problems.
Torticollis
- Torticollis results in a fixed or dynamic posturing of the head and neck in tilt, rotation, and flexion. [1] Spasms of the sternocleidomastoid, trapezius, and other neck muscles, usually more prominent on one side than the other, cause turning or tipping of the head
- Torticollis is not a diagnosis but a symptom of diverse conditions.
- Presentations of torticollis or cervical dystonia are often defined using causal terms
- acute torticollis
- can be the result of blunt trauma to head and neck, or from simply sleeping in an awkward position medications: phenothiazines, metoclopramide, haloperidol, carbamazepine, phenytoin
- may be self-limited in days to weeks
- congenital torticollis
- chronic torticollis/acquired torticollis
- Atlantoaxial rotary subluxation – occurs after minor trauma, pharyngeal surgery, an inflammatory process, or upper respiratory tract infection. It is thought to be precipitated by retropharyngeal edema leading to laxity of ligaments and structures at the atlantoaxial level, permitting the rotational deformity.
- idiopathic or secondary
- Benign paroxysmal torticollis
- a self-limited condition common in infants characterized by repetitive episodes of head tilting with vomiting, pallor, irritability, ataxia, or drowsiness and usually presents in the first few months of life. Episodes can alternate sides.
- acute torticollis
- Differentials:
- Spinal deformity: Early childhood “dropped head syndrome” seen in myopathies and myasthenia, may mimic anterocollis
- Juvenile cerebral palsy with cervical dystonia
- Phenothiazine-induced acute dystonic reactions of childhood
- Juvenile-onset Wilson disease: Often dystonic rather than dyskinetic
- Juvenile-onset Huntington disease: Often dystonic and cervical
- Acquired dystonia of childhood, such as hematoma or other tumor of sternocleidomastoid muscle
- Radiculopathy
- C1 and C2 fractures
- Emergent Management of Myasthenia Gravis
- Multiple Sclerosis
- Neuroleptic Agent Toxicity
- Parkinson Disease
- Peritonsillar Abscess
- Rehabilitation and Cerebral Palsy
- Retropharyngeal Abscess
- Spinal Hematoma
- Tardive Dyskinesia
- Conservative Management
- Anticholinergics (eg, trihexyphenidyl, benztropine) may be somewhat effective but are typically less so than in generalized or torsion dystonias.
- Botulinum toxin injection
- clonazepam, if blepharospasm is part of the syndrome
- baclofen, if oromandibular dystonia is part of the syndrome.
- NSAIDs
- Muscle relaxation techniques
Whiplash
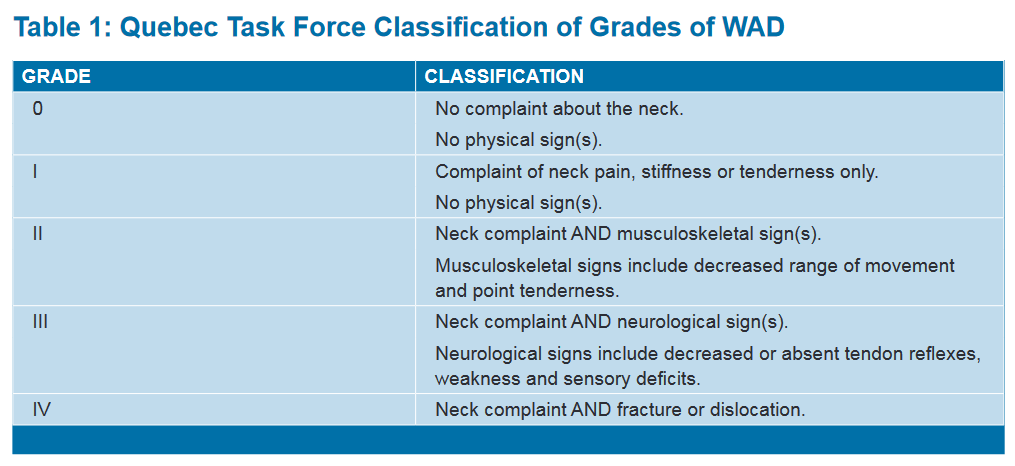
WAD (Whiplash-Associated Disorders)
- The clinical classification of grades of WAD provided by the QTF is shown in the table below. Symptoms and disorders that can manifest in all grades include deafness, dizziness, tinnitus, headache, memory loss, dysphagia and temporomandibular joint pain
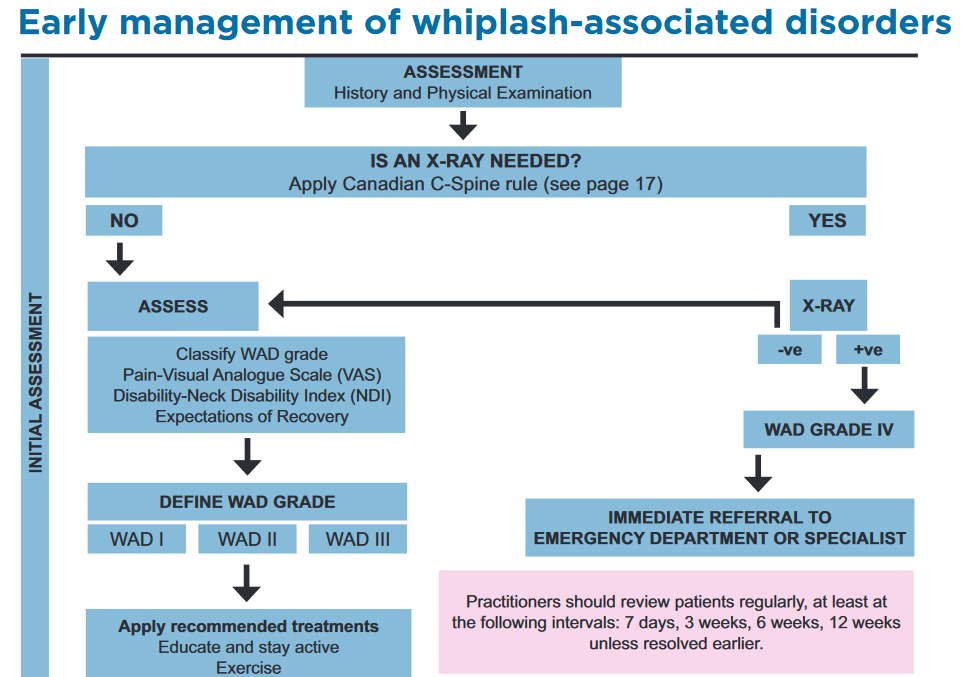
Assessment and diagnosis
- take a history
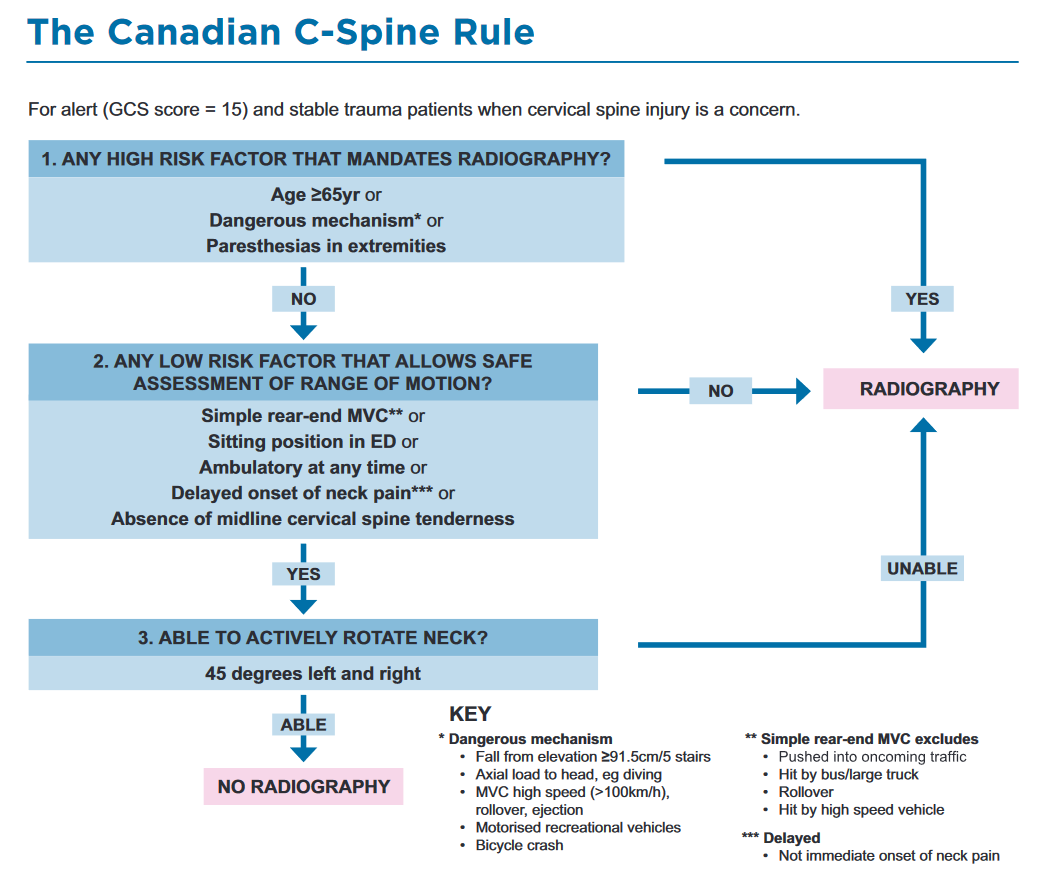
- use the Canadian C-Spine Rule to:
- determine whether X-ray of the cervical spine is required for diagnosis of fracture or dislocation and to avoid unnecessary exposure to X-rays.
- Assess
- WAD grade using the Quebec Task Force Classification (QTF)
- pain using the Visual Analogue Scale (VAS)
- disability using the Neck Disability Index (NDI).
- Expectation of recovery
- can be assessed by simply asking a patient, “Do you think you are going to get better soon?”
- focused physical examination:
- observation (particularly of head position/posture)
- palpation for tender points
- assessment of range of motion (ROM) including flexion (chin to chest), extension, rotation and lateral flexion
- neurological testing
- assessment of associated injuries
- assessment of general medical condition(s), including psychological state
- Imaging
- Based on Canadian C spine Rules
- Do not use MRI or CT in WAD grades I and II.
- Only use CT/MRI with selected patients with WAD grade III, (example P suspected nerve root compression or spinal cord injury)
- Reassure patients that changes (including degenerative or other minor pathological changes) on X-ray, MRI and CT are NOT associated with ongoing pain and disability following WAD
Review
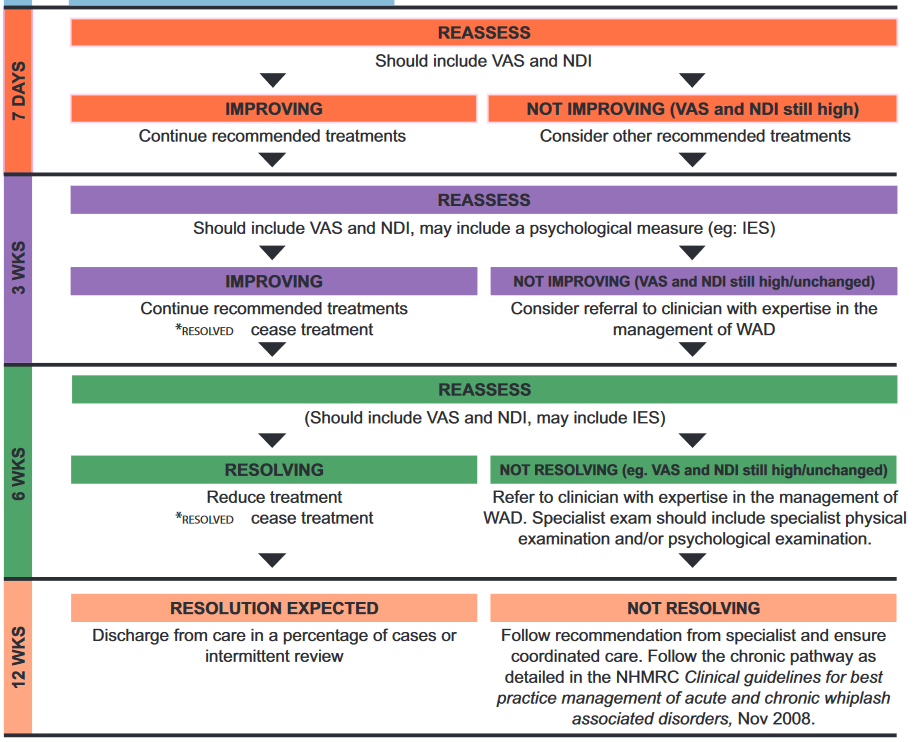
Health professionals should review patients regularly, at least at the following intervals:
- seven days
- three weeks
- six weeks
- three months (unless resolution has occurred earlier)
- Review should include reassessment of the VAS and the NDI.
- A patient is considered to have improved if there is at least a reduction of 10 per cent on these scales.
- Seven-day reassessment
- Reassess using the VAS and NDI.
- If the VAS and NDI are high or unchanged, treatment type and intensity should be reviewed and other recommended treatment options should be considered.
- This may involve referral for physical therapy.
- The effectiveness of such treatments should be closely monitored and only continued if there is evidence of benefit (at least 10 per cent reduction in VAS and NDI).
- Three-week reassessment
- Reassess using the VAS and NDI. If the VAS and NDI are unchanged, a more complex assessment may need to be considered and treatment type and intensity should again be reviewed.
- If the VAS and NDI are unchanged, consider referral to a clinician with expertise in the management of WAD.
- specialist physiotherapist
- specialist chiropractor
- musculoskeletal medicine practitioner
- rehabilitation physician
- pain medicine specialist
- psychologist or occupational physician.
- Amongst other things, if the VAS and NDI are unchanged, the clinician should undertake a more complex physical and/or psychological examination.
- Six-week reassessment
- Reassess again at this point.
- There should be some resolution of symptoms in at least 40% of cases. – treatment should be gradually withdrawn.
- At this point, referral to a psychologist should also be considered.
- This is particularly important if the results of the psychological assessment indicate concern (IES score >25 at the six week reassessment).
- 12-week reassessment
- There should be complete resolution of symptoms in at least 40%.
- in resolving cases, the patient should be reviewed intermittently over the next six to 12 months until resolution, to ensure home programs are maintaining improvement.
| predictive of ongoing pain and disability | NOT predictive of predictive of ongoing pain and disability |
| decreased initial neck range of motion and initial cold hyperalgesia VAS score greater than 5/10 NDI score greater than 15/50 Self-rated collision severity | pain or general physical health status prior to the collision. age, gender, marital status and education seat belt use, awareness of impending collision, position in vehicle and speed of collision high health care utilization for treatment of WAD |
Prognosis
- Provide more concerted treatment or consider earlier referral to a clinician with expertise in the management of WAD for patients with any of the following:
- pain intensity (for example pain >5/10 on VAS scale)
- disability related to neck pain (for example NDI >15/50).
- Reassure patients that changes (including degenerative or other minor pathological changes) on X-ray, MRI and CT are NOT associated with ongoing pain and disability following WAD.
- Practitioners should screen for posttraumatic stress (PTS) symptoms using the Impact of Events Scale (IES), at 3 to 6 weeks post injury.
- Refer patients with IES scores >25 (indicating moderate levels of symptomatology) to a psychologist with expertise in the management of PTS symptoms.
Recommended treatment
- Reassure and stay active.
- Return to usual activities.
- Range of motion, low load isometric, postural endurance and strengthening exercises.
- pain relieving medications:
- Simple analgesics – Paracetamol
- Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
- Opioid analgesics
- Oral opioids, preferably short-acting agents at regular intervals, may be necessary to relieve severe pain in the treatment of acute WAD.
- Ongoing need for such treatment requires reassessment
- Kinesio taping
- trigger point needling
- Manual Therapy:
- manipulation and mobilization of the neck and spine to reduce pain and improve function.
- Exercise Therapy:
- range-of-motion exercises
- strengthening exercises for the cervical spine.
- activity modification:
- ergonomic recommendations to avoid further strain on the neck.
- Posture training
- Training to improve posture can be beneficial, especially for those who have prolonged sitting jobs or poor ergonomic setups.
- Neck Braces or Collars:
- Although their use is sometimes controversial, soft cervical collars may be used in the acute phase for comfort and support.
- NO EVIDENCE – TREATMENTS WHERE THERE IS NO EVIDENCE FOR OR AGAINST THEIR USE
- Traction/ Pilates / Massage / Homeopathy / Cervical pillows / Magnetic necklaces / Heat / Ice / TENS
- TREATMENTS NOT RECOMMENDED
- Reduction of usual activities
- Immobilisation – collars
- Pharmacology – anti-convulsants, anti-depressants
- Muscle relaxants
- Botulinum toxin type A
- Injections – steroid injections
- Pulsed Electromagnetic Treatment (PEM)