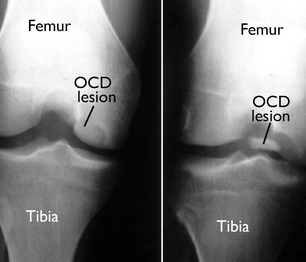
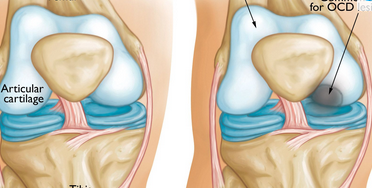
Commonly in boys 5-15yo where a segment of cartilage of the femoral condyle undergoes necrosis, and eventually separates to from an intra-articular loose body
SSx
pain – dull ache worse with activity, improves with rest
Persistent or intermittent joint effusion
restricted ROM
Locations:
knee (most common) – posterolateral aspect of medial femoral condyle (70% of lesions in knee)
capitellum of humerus
talus
Suspect in children if knee pain persists, particularly in the presence of an effusion
younger age correlates with better prognosis, Adult form worse prognosis
open distal femoral physes are the best predictor of successful non-operative management
Nonoperative:
restricted weight bearing and bracing: 50-75% will heal without fragmentation