Scaphoid Fracture
Anatomy and Ossification:
- The scaphoid is one of eight carpal bones in the wrist.
- Ossification begins around the 4th year, possibly earlier in females.
- Approximately 75% of the arterial supply is from branches of the radial artery through vascular perforations on the dorsal surface near the tubercle and waist.

- As vascular supply to the proximal pole is mainly retrograde, a fracture through the waist places the proximal pole at risk of avascular necrosis.
- As such, fractures to this area or more proximally can cause poor outcomes if not managed appropriately.
- Mismanaged fractures can cause malunion and necrosis to the proximal end of the bone and in turn cause instability of the wrist joint.
Whilst immobilisation of scaphoid fractures has traditionally been in a thumb spica, there is good evidence to show that immobilisation of the wrist alone in a short-arm cast is just as effective in promoting union and preventing avascular necrosis.
Prevalence and Causes:
- More common in adolescents than younger children.
- Usually occur from a fall on an outstretched hand
Classification:
- By location: Proximal third, Middle third, Distal third, articular surface, or tubercle.
- waist -65%
- proximal third – 25%
- distal third – 10%
- By orientation: Transverse, vertical, or oblique.
- Displaced or non-displaced.

Clinical Examination:
- Tenderness in the anatomical snuffbox.
- Pain on axial loading of the thumb.
- Limited wrist motion – wrist pain with circumduction
- rarely any ecchymosis, hematoma, or gross deformity
 |  |
| anatomic snuffbox tenderness dorsally | scaphoid tubercle tenderness volarly |
Radiological Investigations:
- Initial test: Plain x-ray with scaphoid views.
- If x-ray is negative but suspicion is high: CT or MRI.
- If further imaging is not immediate, immobilize and arrange early follow-up.
X-Ray Appearance:
- Fractures might not always be visible on initial x-rays.
- if radiographs are negative (27%) and there is a high clinical suspicion
- repeat radiographs in 14-21 days
Other Investigations:
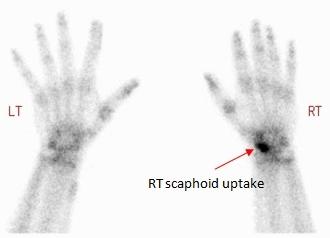
- Bone scan
- MRI
- indications
- sensitivity and specificity
- approach 100% for occult fractures
- CT scan with 1mm cuts along scaphoid axis
- indications
- sensitivity and specificity
- 62% sensitivity and 87% specific for determining stability and fracture
- less effective than bone scan and MRI to diagnose occult fracture
{kind=link}
{kind=link}
{kind=link}
Reduction Requirements:
- Scaphoid fractures rarely require acute reduction in the ED.
- Exception: Trans-scaphoid peri-lunate fracture-dislocations.
Orthopedic Referral:
- Urgent referrals are rare, except for open injuries or dislocations.
- Typical referral for fracture clinic review within 1-2 weeks.
ED Management:
- Immobilization in either a short-arm cast or a thumb spica.
- Referral for fracture clinic follow-up.
- Re-evaluate with repeat x-ray or MRI as needed.
Immobilization Options:
- Short-arm cast
- thumb spica cast – in wine glass holding position


 |  |
Parental Advice:
- Stress the importance of follow-up and keeping the cast on until review.
- Explain the high likelihood of union with early and appropriate management.
Potential Complications:
- Scaphoid Nonunion
- incidence: 5-10% following immobilization, higher rates for proximal pole fractures
- risk factors: vertical oblique fracture pattern, displacement >1mm, advancing age, nicotine use
- treatment: vascularized or nonvascularid bone grafting procedures
- Osteonecrosis
- 13-50% of all scaphoid fractures
- many studies showing 100% in proximal fifth fractures with immobilization
- Malunion
- flexion of distal fragment and extension of proximal fragment due to pull of scapholunate interosseous ligament creating shortened bone with humpback deformity
- treatment: no clear indications supporting operative versus non-operative treatment
- Subchondral bone penetration with arthrosis due to prominent hardware
- seen following mini-open fixation techniques
- incidence has decreased with use of fluoroscopy
- treatment: revision surgical fixation versus implant removal following union
- SNAC wrist (scaphoid nonunion advanced collapse)
