First time seizure
Differentials
“SICK DRIFTER”
- Substrates (sugar, oxygen)
- Isoniazid overdose
- Cations (Na, Ca, Mg)
- Kids (eclampsia)
- Drugs (CRAP: Cocaine, Rum (alcohol), Amphetamines, PCP)
- Rum (alcohol withdrawal)
- Illnesses (chronic seizure disorder or other chronic disorder)
- Fever (meningitis, encephalitis, abscess)
- Trauma (epidural, subdural, intraparynchymal hemorrhage)
- Extra: toxocologic (TAIL: Theo, ASA, Isoniazid, Lithium) and 3 Anti’s: (Antihistamine overdose, Antidepressant overdose, Anticonvulsants (too high dilanitin, tegretol) or benzo withdrawal.
- Rat poison (organophospates poisoning – not actually rat poison!)
| Medications (partial list) | Vital Signs | Metabolic |
| Bupropion, Camphor, Clozapine, Cyclosporine, Fluoroquinolones, Imipenem, Isoniazid, Lead, Lidocaine Lithium, Metronidazole, TheophyllineTCAs , Baclofen | Hypoxia Hyperthermia HTN Emergency | Hepatic Encephalopathy Uremia Hypoglycemia Hyperglycemia |
| Withdrawal Syndromes | Infectious | CNS Abnormalities |
| Alcohol AEDs Benzoz | Encephalitis CNS Abscess Meningitis | Traumatic Brain Injury TIA SAH CVA Traumatic ICH SOL (i.e. Tumor) |
| Electrolytes | mimic seizures | Pseudoseizures |
| Hypocalcemia Hypercalcemia Hyponatremia Hypomagnesaemia | Eclampsia Migraine prodrome Nonepileptic seizures/ pseudoseizures Syncope Acute dystonic reactions Rigors Narcolepsy & sleeping disturbances Cardiac disorders (e.g. Dysrhythmias, Long QT syndrome, HOCM) | volitional or non-volitional preserved consciousness or purposeful movements asymmetric movements poorly coordinated thrashing back arching eyes held shut head rolling pelvic thrusting bicycling/ pedalling movements of legs |
| Distinguishing features | Seizure | Syncope |
| Immediate precipitating factors | Usually none | Emotional stress, Valsalva, Orthostatic hypotension, Cardiac aetiologies |
| Premonitory symptoms | None or aura | Tiredness, nausea, diaphoresis, tunnelling of vision |
| Posture at onset | Variable | Usually erect |
| Transition to unconsciousness | Often immediate | Gradual – over secs (may be sudden with cardiac arrhythmias) |
| Duration of tonic-clonic mvts | 30 – 60 secs | < 15 secs |
| Facial appearance during event | Cyanosis, frothing at mouth | Pallor |
| Disorientation & sleepiness after event | Many mins – hrs | < 5 mins |
| Aching of muscles after event | Often | Sometimes |
| Biting of tongue | Sometimes | Rarely |
| Incontinence | Sometimes | Sometimes |
| Headache | Sometimes | Rarely |
Approach
- Is the patient back to his baseline neurological status?
- Get collateral information to ensure an accurate answer
- Is this a first time seizure?
- Be aware that 50% of “first time seizures” have had prior events
- Consider Syncope!
- Is the seizure provoked or unprovoked?
- Provoked seizure:
- An acute symptomatic seizure that occurs at the time of or within 7 days of an acute neurologic, systemic, metabolic, or toxic insult (Huff 2014).
- Unprovoked seizure:
- A seizure occurring in the absence of acute precipitating factors and includes remote symptomatic seizures, as well as seizures that are not established to have a cause.
- Provoked seizure:
Investigations
Bedside
- glucose
- blood gas/ lactate
Laboratory
- UEC, CMP (Na+, glucose, Ca2+, renal function)
- toxins (TCA, theophylline, amphetamines, other recreational drugs, salicylates, glycols, alcohols, hydrocarbons)
- Prolactin levels (peak at 20 minutes after seizure, return to baseline in 60 minutes)
- TFTs
Imaging
- Non-Contrast Head CT (NCHCT) (Rosen’s 2014)
- Unprovoked, back at baseline:
- NCHCT not indicated
- Provoked or unprovoked, NOT at baseline:
- Obtain NCHCT
- NCHCT abnormal in up to 80% of patients with focal neurological deficit after seizure (Harden 2007)
- Provoked and back at baseline:
- No definitive recommendations
- NCHCT unlikely to have high-yield
- If provoking factor addressed and patient can reliably follow up, may consider outpatient imaging
- Unprovoked, back at baseline:
- Electroencephalogram (EEG)
- Provoked or unprovoked, NOT at baseline = Emergent EEG
- Concern for status (nonconvulsive) epilepticus
- Mortality rates estimated to be as high as 40% (Tardy 1995)
- If patient returns to baseline, EEG can be deferred to outpatient
- ECG
- Always obtain an ECG in first time seizure patients
- The challenge:
- Significant overlap in presentation with syncope often having myoclonic or tonic jerks (12-75%) due to cerebral hypoperfusion (Bergfeldt 2003)
- The importance:
- Misdiagnosing syncope as seizure can lead to application of incorrect treatment and, thus mortality and morbidity
- Can’t miss EKG findings (Bergfeldt 2003)
- Wolff-Parkinson-White syndrome
- Prolonged QT interval (especially in younger patients)
- Brugada syndrome: RBBB pattern with STE in V1-V3
- Hypertrophic cardiomyopathy
- Arrhythmogenic RV dysplasia: Negative T waves in V1-V3 with or without epsilon waves
- Bi/tri fascicular blocks or undetermined intraventricular conduction abnormalities
- High degree AV blocks
- Lumbar Puncture
- Indicated if there’s a concern for a CNS infection (i.e. meningitis, encephalitis)
- Lower threshold to LP if patient is immunocompromised (increased rate of CNS toxoplasmosis, CNS abscess etc)
- Provoked or unprovoked
- At baseline: No LP
- NOT at baseline: Obtain LP
Management Goals
1. Resuscitation to prevent secondary brain injury and maintain cerebral perfusion pressure
2. Terminate seizure
3. Decrease cerebral metabolic rate
4. Diagnose and treat cause
5. Treat complications
Resuscitation
- Attend to ABCS and address life threats
- Manage airway with recovery position, airway adjuncts and intubation if required
- Optimise oxygenation and provide ventilatory support as needed (prone to hypercapnia)
- Early IV or IO access, optimise cerebral perfusion pressure
- Treat hypoglycaemia and life-threatening electrolyte disturbance if present
- Maintain normothermia
- Give relevant antidote if due to toxic agent (e.g. pyridoxine for isoniazid)
Terminate seizure
- First line therapies
- Bolus dose benzodiazepines
- Midazolam 0.1mg/kg IV – also buccal or IM (IM not inferior to IV lorazepam)
- Lorazepam 0.1mg/kg IV (onset in 3-5 minutes and last hours; preferred for longer acting effects)
- Diazepam 5mg IV/PR (avoid IM as painful) (onset in ~1 minute but lasts only about ~20 min for anticonvulsant activity)
- Clonazepam
- Bolus dose benzodiazepines
- Second line therapies (typically requires intubation and mechanical ventilation)
- Phenytoin 15-20 mg/kg IV over 30 minutes or longer
- should not be used to terminate seizures as a sole agent, always with benzodiazepines
- some regard phenytoin as a first line therapy, however not all seizures require therapy in addition to termination with benzodiazepines
- avoid if usually on phenytoin
- avoid rapid push to risk of cardiovascular toxicity from the propylene glycol diluent
- fosphenytoin is not available in Australia
- Valproic acid — 40 mg/kg IV over 10 min (may give additional 20 mg/kg over 5 min if still seizing)
- Leviteracetam (off label use for status epilepticus)
- Phenytoin 15-20 mg/kg IV over 30 minutes or longer
- Third line therapies (for refractory status epilepticus; typically require intubation and ventilation and cEEG monitoring)
- propofol 2-3mg/kg IV then <4mg/kg/hr
- midazolam IV infusion
- Barbiturates
- Phenobarbitone infusion 10mg/kg IV boluses -> 0.2-0.4mg/kg/min
- Thiopentone 4mg/kg IV (then repeat boluses or infusion targetting burst suppression)
- Clonazepam IV infusion
- Fourth line therapies
- Thiopentone (if not already started)
- Volatile anaesthetic agent (e.g. isoflurane)
- Ketamine infusion
- Magnesium
- Lignocaine
- Other seizure therapies of uncertain efficacy
- steroids
- immunomodulation (IV IgG or plasmapheresis)
- ketogenic diet
- hypothermia
- deep brain stimulation
- surgical interventions
- Monitor for ongoing seizures
- Avoid neuromuscular blockade, consider using suxamethonium for intubation due to short duration of effect (~10 minutes)
- Observe for muscular activity
- cEEG to exclude non-convulsive status epilepticus in patients who do not return to normal conscious state
- A period of 24–48 h of electrographic control is recommended prior to slow withdrawal of continuous infusion AEDs for RSE
Treat underlying cause
- Antibiotics – bacterial infection
- Antivirals – viral infection
- Abscess – surgery
- Increased ICP – neurosurgical decompression
- Eclampsia – Mg2+ and BP management (early delivery of baby and placenta)
- Isoniazid OD or pyridoxine-dependent seizures (e.g. neonates) – pyridoxine
- Cholinergic syndrome – atropine, palidoxime if organophosphate poisoning)
- Sodium channel blocker overdose – sodiu bicarbonate, intralipid
Restore
- Ensure patient receives normal therapeutic prophylaxis
- Check levels
- Consider adding a new generation in difficult cases
Prevent and treat complications
- aspiration
- neurogenic pulmonary oedema
- rhabdomyolysis
- hyperthermia
- trauma (e.g. head injury due to fall, posterior shoulder dislocation)
- Todd’s paralysis (may last 24h)
Disposition
- Patients with status epilepticus generally require HDU/ ICU admission
- Neurology consult
PROGNOSIS
- prolonged seizures have higher mortality and worse outcomes
- mortality of status epilepticus ranges from ~ 10-30% in different studies, depending on the definition used
OTHER INFORMATION
- non-IV benzodiazepines (e.g. IM midazolam) are often preferred first-line therapy in prehospital settings
- respiratory decompensation is more commonly encountered in untreated status epilepticus than in status epilepticus treated with benzodiazepines
- Titrate AEDs to therapeutic levels. When checking post-load drug levels, on should wait at least 2 hours post infusion for fosphenytoin and phenytoin, or immediately post infusion of valproate
- Phenytoin is typically avoided in drug-induced seizures, barbiturates are widely recommended following first line benzodiazepine therapy
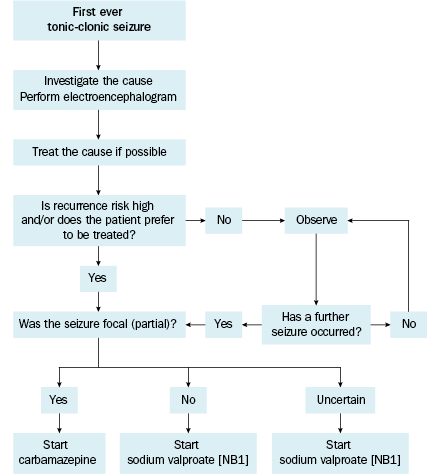
- Current best literature does not uniformly recommend starting AEDs after a first time seizure (Knake 2009)
- Early treatment does not seem to provide protection from future seizures.
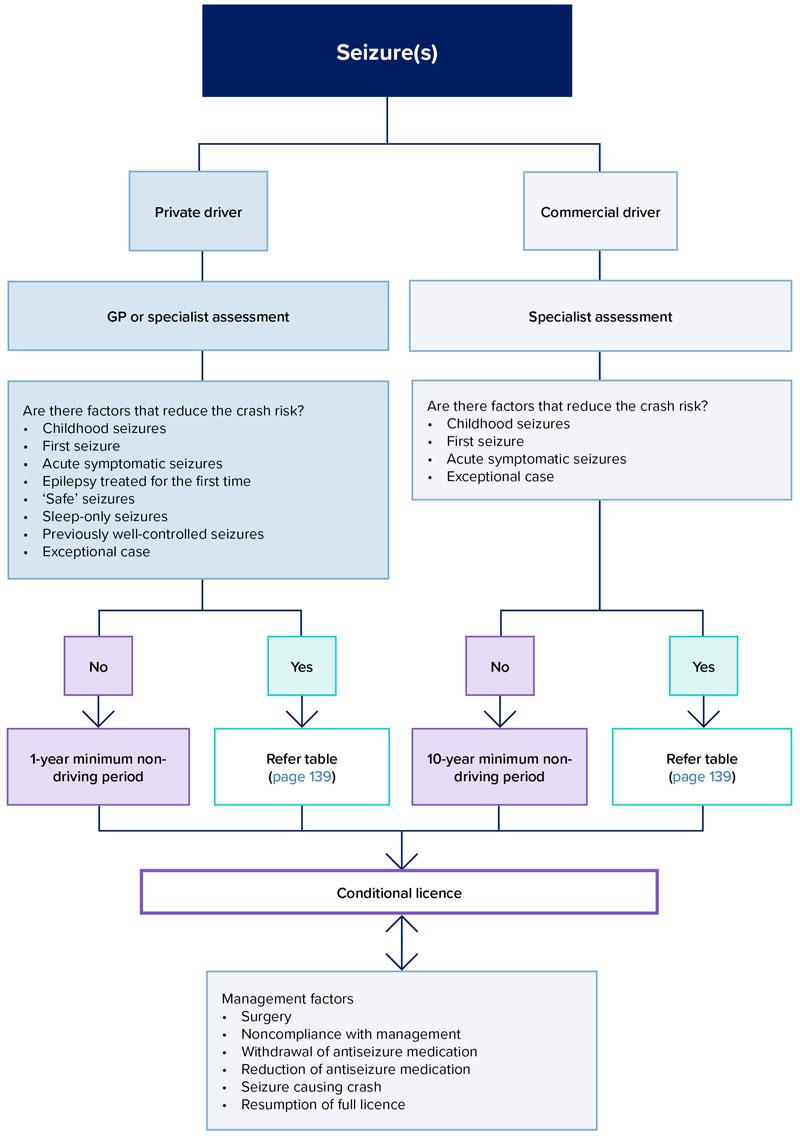
Driving standards
The first seizure (of any type)
- The occurrence of a first seizure warrants medical specialist assessment, where available.
- Approximately half of all people experiencing their first seizure will never have another seizure, while half will have further seizures (i.e. epilepsy). The risk of recurrence falls with time.
- Driving may be resumed after sufficient time has passed without further seizures (with or without medication) to allow the risk to reach an acceptably low level
- Note: Two or more seizures in a 24-period are considered a single seizure
- conditional licence – Private standards
- there have been no further seizures (with or without medication) for at least 6 months
- subject to at least annual review
- unconditional licence
- antiseizure medication has not been prescribed in the past 12 months; and
- there have been no seizures for at least 2 years.
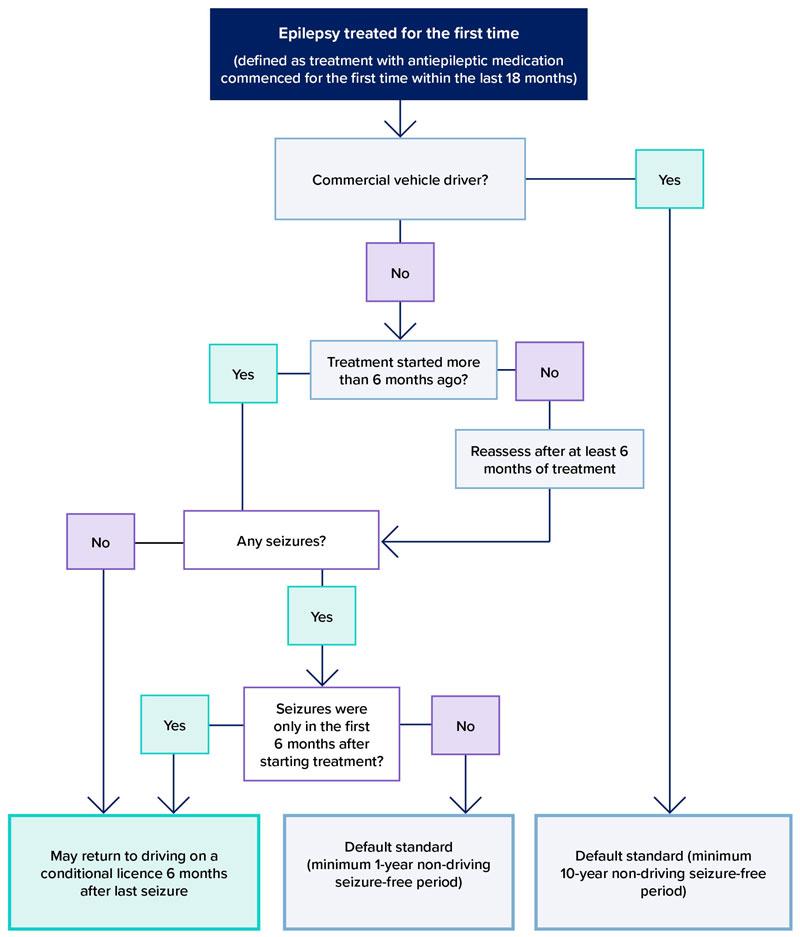
Epilepsy treated for the first time – Private standards
- This applies when antiepileptic treatment has been started for the first time within the preceding 18 months.
- conditional licence
- the person has been treated for at least 6 months; and
- there have been no seizures in the preceding 6 months; and
- if any seizures occurred after the start of treatment, they happened only in the first 6 months after starting treatment and not in the last 6 months; and
- the person follows medical advice, including adherence to medication.
- subject to at least annual review
Medication noncompliance
- if suspects noncompliance, can recommend to the driver licensing authority that the license be granted on the condition that periodic drug-level monitoring is conducted.
- Where a person without a history of noncompliance with medication
- experiences a seizure because of a missed dose +
- there were no seizures in the 12 months leading up to that seizure
- the situation can be considered a provoked seizure