Seizures
- Epilepsy = at least two unprovoked seizures occurring more than 24 hours apart
- Complex = any impact on consciousness
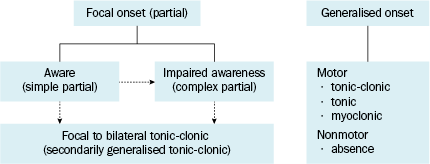
Classification of Seizures (isuri notes…)
- Partial seizures (seizures beginning focally → seizure activity is restricted to discrete areas of the cerebral cortex e.g. due to a structural abnormality)
- Simple partial seizures – consciousness not impaired
- with motor symptoms
- with somatosensory or special sensory symptoms e.g. taste/smell
- with autonomic symptoms
- with psychological symptoms e.g. jamais vu or deja vu
- Complex partial seizures – with impairment of consciousness
- Beginning as a simple partial seizure & progressing to a complex partial seizure
- Altered LOC at onset
- Partial seizures with secondary generalisation
- Generalised seizures (involve diffuse areas of the brain simultaneously → e.g. due to widespread cellular, biochemical or structural abnormalities)
- Absence seizures
- Typical (petit mal)
- Atypical
- Others
- Tonic-clonic seizure (grand mal)
- Tonic seizure
- Clonic seizure
- Atonic
- Myoclonic
- Unclassified seizures
- Neonatal seizures
- Infantile spasms
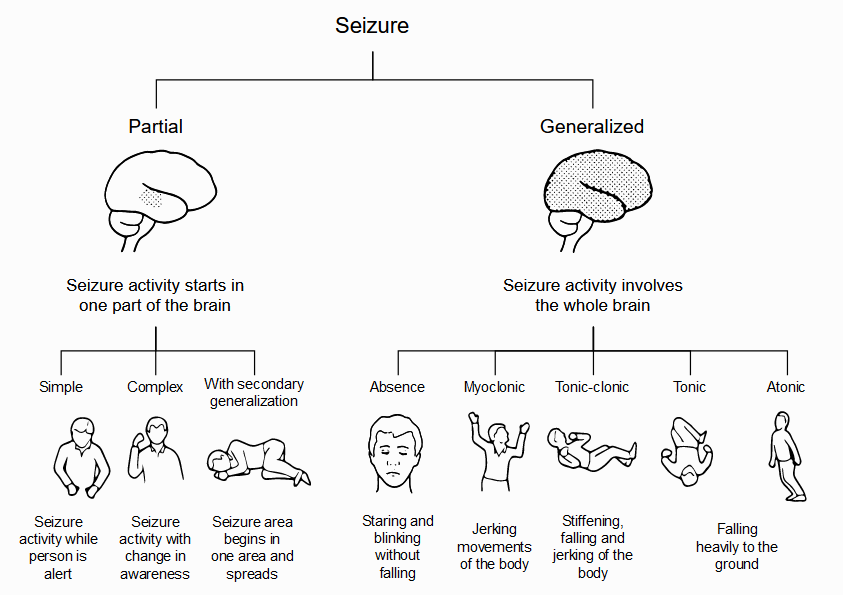
Partial Seizures – occur within discrete regions of the brain
Simple Partial Seizures (jaksonian epilepsy)
- Consciousness is fully preserved during the seizure & clinical manifestations are relatively simple
- Can get motor, sensory, autonomic or psychiatric symptoms
- Motor
- Involuntary hand movements e.g. mvts in (L) arm with seizure arising from the (R) primary motor cortex
- Clonic – repetitive flexion/extension movements (~2-3Hz)
- Additional features of partial motor seizures
- Involuntary mvts may begin in restricted regions (e.g. fingers) & quickly spread to larger portions of the extremity → ‘Jacksonian march’
- Localised paresthesia (Todd’s paralysis) – for mins-hrs following the seizure
- Epilepsia Partialis Continua – seizures continue for hrs-days (refractory to medical Tx)
- Involuntary hand movements e.g. mvts in (L) arm with seizure arising from the (R) primary motor cortex
- Sensory
- Paresthesia
- Vision: flashing lights, formed hallucinations
- Equilibrium: sensation of falling, vertigo
- Hearing: unusual sounds
- Olfaction: unusual, intense odours
- Autonomic
- Sweating
- Flushing
- Piloerection
- Psychological
- Fear
- Sense of impending change
- Detachment
- Depersonalisation
- Déjà vu
- Illusions that objects are growing smaller (micropsia) or larger (macropsia)
Complex Partial Seizures
- Consciousness is impaired & clinical manifestations are more complex
- Characterised by focal seizure activity accompanied by a transient impairment of the pt’s ability to maintain normal contact with the environment
- Pt is unable to respond to visual or verbal commands during the seizure
- Pt has impaired recollection or awareness of the ictal phase
- Seizure frequently begins with an aura e.g. a simple partial seizure
- Ictal phase:
- Sudden behavioural arrest or motionless stare
- marks onset of the period of amnesia
- Automatisms – involuntary, automatic behaviours
- Chewing
- Lip smacking
- Swallowing
- Picking mvts of the hands
- Display of emotions
- Running
- Sudden behavioural arrest or motionless stare
- Following the seizure:
- Pt is often confused
- Transition to full recovery of consciousness can vary from seconds – 1hr
- + anterograde amnesia
- + postictal aphasia in cases involving the dominant hemisphere
- Interictal (btw seizures) EEG: often normal
- May show brief discharges (epileptiform spikes or sharp waves)
Partial Seizures with Secondary Generalisation
- Partial seizures can spread to involve both hemispheres → generalised seizures (usually tonic-clonic)
- Secondary generalisation is frequently observed following simple partial seizures
- Often the focal onset of the seizure is only evident on careful Hx → identifies a preceding aura (simple partial seizure)
Generalised Seizures – arise from both cerebral hemispheres simultaneously
Absence Seizures (Petit Mal)
- Sudden brief lapses of consciousness without loss of postural control
- Can be accompanied by subtle, bilateral motor signs
- Rapid blinking of eyelids
- Chewing mvts
- Small-amplitude clonic mvts of the hands
- Can be accompanied by subtle, bilateral motor signs
- Lasts for a few seconds
- Consciousness returns suddenly
- No postictal confusion
- Seizures can occur hundred times/day
- Child may be unaware or unable to convey their existence
- Usually begin in childhood (4 – 8) or early adolescence
- Main seizure type in 15-20% of children with epilepsy
- Often not recognised early due to subtle symptoms
- Can be reported as ‘daydreaming’ or a deterioration in school performance
- EEG:
- Generalised, symmetric, 3-Hz-spike-and-wave discharge → often corresponds to clinical signs
- Begins & ends suddenly
Atypical Absence Seizures
- Present with features that deviate both clinically & electrophysiologically from typical absence seizures
- Change in LOC
- Longer lasting
- Less abrupt in onset & cessation
- Seizure accompanied by more obvious motor signs (focal or lateralising features)
- Associated with diffuse or multifocal structural abnormalities of the brain → may accompany other signs of neurological dysfunction
- Less responsive to anticonvulsants (when compared with typical absence seizures)
| Clinical Feature | Absence Seizures | Complex Partial Seizure |
| Frequency | Multiple | Uncommon > 2/day |
| Duration | Usually < 10s; rarely > 30s | Usually > 1min |
| Aura | Never | Frequently |
| Onset/Termination | Abrupt | Gradual |
| Post-ictal | Resume preictal state of mind/activity | Confusion, fatigue |
| Automatisms | Common | Frequently |
| Eye Blinking | Common | Occasionally |
| Seizures activated by:HyperventilationPhotic stimulation | Very frequentlyFrequently |
Occasionally Rarely |
| EEGIctalInterictal | Generalised spike & wave (3Hz)Usually normal |
Uni-/bi-lateral temporal/frontal dischargesVariable: spikes/ waves in frontal/temporal lobes |
| Antiepileptics | ValproateEthosuximide | CarbamazepineOxcarbazepine → both worsen absence seizures |
Generalised, Tonic-Clonic Seizures (Grand Mal)
- Main seizure type in ~10% of ppl with epilepsy
- Most common seizure type resulting from metabolic disturbances
- Seizure – Ictal phase
- Begins abruptly without warning
- Some pts describe vague premonitory symptoms – these prodromal symptoms are distinct from stereotypic auras
- Tonic phase – initial phase
- Tonic contraction of muscles through the body
- Muscles of expiration & larynx
- Tonic contraction of muscles through the body
- Begins abruptly without warning
| → loud moan or ‘ictal cry’→ impaired respiration | → pooling of secretions in the oropharynx→ cyanosis |
- Jaw muscles
- → biting of tongue
- ↑sympathetic tone
- → ↑HR
- → ↑BP
- → ↑pupillary size
- EEG:
- progressive increase in generalised low-voltage fast activity
- followed by high-amplitude, polyspike discharges
- Switches to the next phase after ~ 10 – 20s
- Clonic phase
- There is superimposition of periods of muscle relaxation on the tonic muscle contraction
- Periods of relaxation progressively increase until the end of the ictal phase (< 1 min)
- EEG:
- High-amplitude activity is interrupted by slow waves → spike & wave pattern
- Post-ictal phase
- Unresponsiveness
- Muscular flaccidity
- Excessive salivation → stridous breathing & partial airway obstruction
- Bladder & bowel incontinence
- Gradually regain consciousness (mins – hrs)
- During this transition there is a period of post-ictal confusion
- Can be very long, esp. with prolonged seizures or underlying CNS disease
- EEG: diffuse slowing – gradually recovers as the pt awakens
- Pts can later C/O:
- Headache
- Fatigue
- Muscle ache – can last for hrs
- There are variations of tonic-clonic seizures:
- Pure tonic seizures
- Last for a few secs
- Pure clonic seizures
- Pure tonic seizures
Atonic Seizures (Drop Attacks)
- Sudden loss of postural muscle tone – lasts 1-2 secs
- Brief seizure → quick head drop or nodding mvt
- Longer seizure → pt will collapse
- N.B. risk of head injury
- Consciousness is briefly impaired
- Usually no post-ictal confusion
- EEG:
- brief, generalised spike & wave discharges
- followed immediately by diffuse slow waves → correlate with the loss of muscle tone
- Usually seen in association with known epileptic syndromes
Myoclonic Seizures
- Sudden & brief muscle contraction that may involve one part of the body or the entire body
- Common physiological form – normal
- Sudden jerking mvt observed while falling asleep
- Pathological myoclonus is seen in association with
- metabolic disorders
- degenerative CNS disorders
- anoxic brain injury
- Due to cortical dysfunction → true epileptic event
- EEG:
- Bilateral synchronous, spike & wave discharges synchronised with the myoclonus
- Coexist with other forms generalised seizure disorders
- Predominant feature of juvenile myoclonic epilepsy
Causes of Seizures According to Age
- Neonates (< 1 month)
- Perinatal hypoxia & ischemia
- Intracranial haemorrhage & trauma
- Acute CNS infection
- Congenital CNS abnormalities
- Metabolic disturbances: hypoglycaemia, hypocalcaemia, hypomagnesemia, pyridoxine (Vitamin B6) deficiency)
- Drug-withdrawal seizures
- Babies who’s mothers used drugs e.g. cocaine, heroin or ethanol → susceptible to withdrawal
- Genetic disorders
- Infants & children (> 1 mth – < 12 yrs)
- Febrile seizures
- Prevalence: btw 3mths – 5 yrs
- Peak incidence: btw 18 – 24mths
- Seizures associated with fever but no evidence of CNS infection or other defined causes
- Genetic disorders
- Metabolic
- Degenerative
- Primary epilepsy syndromes
- CNS infection
- Developmental disorders
- Trauma
- Idiopathic
- Febrile seizures
- Adolescents (12 – 18 yrs)
- Trauma
- Genetic disorders
- Infection
- Brain tumour
- Illicit drug use
- Idiopathic
- Young adults (18 – 35 yrs)
- Trauma
- Alcohol withdrawal
- Illicit drug use
- Brain tumour
- Idiopathic
- Older adults (> 35 yrs)
- Cerebrovascular disease
- Brain tumour
- Alcohol withdrawal
- Metabolic disorders
- Uraemia
- Hepatic failure
- Electrolyte abnormalities
- Hypoglycaemia
- Alzheimer’s disease & other degenerative CNS diseases
- Idiopathic
CLINICAL FEATURES
History
- description of seizure activity
- time of onset and offset
- warning signs
- parts of body involved in motor activity, and sequence of involvement
- history of epilepsy
- family history
- compliance
- precipitants
- drug withdrawal
- intercurrent illness
- new medications (e.g. antipsychotics, antidepressants, isoniazid)
- recreational drug use (e.g. sympathomimetics)
- traumatic brain injury
Examination
- observation of seizure activity if persists
- temperature
- meningism
- focal neurology
- pupils (response to light is ‘poor man’s EEG’)
- general examination
- lateral tongue biting
- incontinence
Management – Starting AEDs
Current best literature does not uniformly recommend starting AEDs after a first time seizure (Knake 2009)
Early treatment does not seem to provide protection from future seizures.
|
Drug / Indication |
Formulations |
Dosing |
Pharmacokinetic Data |
|
Carbamazepine (Tegretol®, Tegretol-XR®, Carbitrol®, )
|
Chewable tabs: 100 mg
|
<6 yrs: Tablets, suspension: Start 5mg/kg PO daily divided BID-QID, increase every 5–7 days to a max of 35 mg/kg/day
|
Half-life: Initially range from 25–65 hrs, decreasing to 12–17 hrs on repeated doses
|
|
Clonazepam (Klonopin®)
|
Tablets: 0.5, 1 and 2 mg
|
Infants and Children: (<10 yrs of age or < 30 kg) Initial dose between 0.01 and 0.03 mg/kg/day divided BID-TID, then increase by 0.25–0.5 mg every 3 days. Maintenance dose range between 0.1 to 0.2 mg/kg. |
Half-life: 30–40 hrs |
|
Diazepam (Valium®)
|
Tablets: 2, 5, and 10 mg
|
Status epilepticus: |
Half-life: 46–71 hrs
|
|
Valproate/divalpro ex sodium (Depakote , Depakene )
|
Delayed-release tablets: 125, 250, and 500 mg
|
Children and adults: (IV) Total daily IV dose is equivalent to the total daily oral dose; IV dose should be divided every 6 hours; switch patients to oral as soon as clinically possible. IV has not been studied for >14 days. |
Half-life: Newborns (1st week of life): 30–60 hrs
|
|
Phenytoin (Dilantin®)
|
Infatabs (chewable): 50 mg
|
Pediatrics: |
Half-life: |
|
Gabapentin (Neurontin®)
|
Capsules: 100, 300, and 400 mg
|
Pediatric dosing: Start 10–20 mg/kg/day, increase by 10 mg/kg/day to a maintenance does of 30 mg/kg/day. Max is 50–100 mg/kg/day in refractory patients. |
Half-life: 5–7 hrs
|
|
Lamotrigine (Lamictal®)
|
Dispersible Tablets: 5 and 25 mg
|
Adding to a regimen containing VPA in 2–12 yrs: Start 0.15 mg/kg/day in divided QD-BID X 2 wks, then increase to 0.3 mg/kg daily divided QD-BID x 2 wks, then increase every 1–2 wks by 0.3 mg/kg/day to a usual maintenance dose of 1–5 mg/kg/day. Max is 200 mg/day divided QD-BID.
|
Half-life: Ages 10 mo-5.3 yrs: 7.7–44.9 hrs
|
|
Levetiracetam Keppra®
|
Tablets: 250, 500 and 750 mg
|
Children: One study used 13–30 mg/kg in 5–12 yo. Data suggested children metabolized drug more quickly than adults. |
Half-life: 6–8 hrs
|
|
Lorazepam (Ativan®)
|
Tablets : 0.5, 1, and 2 mg
|
Status Epilepticus: |
Half-life: 12 hrs
|
|
Midazolam (Versed®)
|
IV: 1 mg/ml and 5 mg/ml
|
6 months to <6 yrs: Syrup:
Status Epilepticus refractory to standard therapy:
|
Half-life: PO: 2.2–6.8 hrs
|
|
Oxcarbazepine (Trileptal®)
|
Tablet: 150, 300, 600 mg
|
Children: Doses Start 8–10 mg/kg, do not exceed 600 mg/day in divided doses. Target dose should be achieved over a 2 week period and is dependent on patient weight.
|
Half-life: 3 to 13 hrs
|
|
Phenobarbital (Luminal®)
|
Tablets: 15, 16, 30, 32, 60, 65, and 100 mg
|
Status Epilepticus: (IV) |
Half-life: |
|
Tiagabine (Gabatril®)
|
Tablets: 2, 4, 12, 16, and 20 mg
|
12–18 yrs: Start 1–3 mg/kg/day PO QHS X 1 wk, increase to 8 mg PO QD on wk 2, then increase by 4–8 mg/wk to a max of 32 mg/day. Total daily dose should be given in divided doses of 2–4 times/day |
Half-life:7–9 hrs
|
|
Topiramate (Topamax )
|
Tablets: 25, 100, and 200 mg
|
2–16 yrs: Start 1–3 mg/kg/day PO QHS X 1 wk. Titrate by 1–3 mg/kg/day divided bid at 1–2 wk intervals. |
Half-life: 21 hrs
|