Tension Headache
- Female predilection not so pronounced as in migraine
- Often begins in young adulthood or later
- characteristics:
- mild to moderate in severity
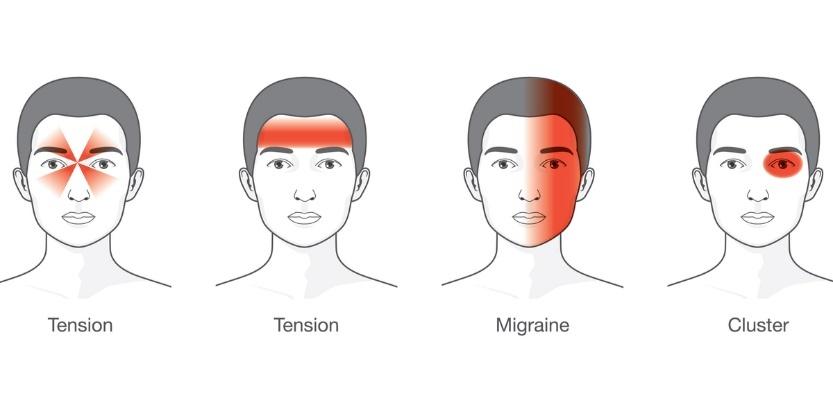
- bilateral 90% of the case
- often felt as a pressure or constriction, felt as a band or concentrated, for example, in the frontal or occipital areas
- not accompanied by significant systemic upset or neurological deficits
- not aggravated by routine physical activity such as walking or climbing stairs
- there is no aura
- but photophobia, phonophobia and nausea may occur
- Episodes
- last from 30 minutes to 7 days
- Nausea or vomiting does not occur
- The spectrum of severity:
- mild and infrequent attacks to daily, almost continuous, pain
- Tension type headaches may be seen together with migraine in some patients with frequent headaches
| Tension-type headaches (50% incidence) | Migraine(25%) | |
| Nature of pain | Non-pulsatile band, Tight gripping pressure, constant, no effect of head movement | Throbbing pulsating worsening of pain with movement |
| Site of pain | Bitemporal, occipital or generalised (may be retro-orbital, may be band-like) | Unilateral (often in temple or retro-orbital) |
| Associated features | Often at end of day Few associated symptoms Possible blurred vision May have nausea (rarely vomits) Usually no: – photophobia – phonophobia – osmophobia May be associated with sleep disturbance. | Teichopsia (zigzag, bright, shimmering lights) Fortification spectra (like top of fortress) Rainbow effect Photons of bright light in visual field Nausea and vomiting Photophobia Phonophobia Osmophobia |
| Precipitating factors | Often at times of stress | altered sleep patterns (too little or too much) overexertion skipping meals changes in stress level excess of afferent stimuli e.g. bright lights changes in the weather may precipitate migraine attacks menstruation |
| Acute intervention | Rest Simple analgesia Alcohol may reduce symptoms | Triptans Ergots Occasional early use analgesics |
| Prophylaxis | Tricyclic antidepressants:amitriptyline if difficulty sleepingimipramine if no problem sleeping | Pizotifen |
Treatment
- general measures
- avoid:
- overwork & stress
- lifestyle changes
- relaxation therapy
- cognitive training
- excess alcohol
- lack of exercise – tension type headache is more commonly seen in sedentary people
- avoid analgesic abuse
- withdrawal of analgesics may cause rebound symptoms for up to 14 days
- 3-week course of naproxen 250-500mg bd, taken regularly, may break the cycle of frequently recurring or unremitting headaches and the habit of responding to pain with analgesics. If it fails, it should not be repeated
- overwork & stress
- Tobacco Cessation
- treat clinical depression/anxiety
- physiotherapy
- massage, mobilization
- manipulation
- correction of posture
- Medications
- Analgesics
- Paracetamol
- NSAIDs
- Aspirin
- Avoid Opioids
- Myofascial injections
- Trigger Point Injection at affected occiput or Lower Cervical Intramuscular Injection
- Selective C1-C2 lateral Joint Injection
- prophylaxis
- Tricyclic Antidepressants
- Amitriptyline
- 10–25 mg nocte up to a maximum of 75 mg
- Doses as high as 200 mg or 250 mg nocte may be required for unremitting headaches
- Tension-vascular headache
- beta-blockers (propranolol)
- 10–40 mg twice daily and titrating up as needed.
- Doses as high as 160 mg four times daily may be required for unremitting headaches
- Amitriptyline
- Tricyclic Antidepressants