Autism spectrum disorders
is a lifelong neurodevelopmental condition features of which become evident in early childhood
They can be more difficult to assess because they communicate differently and may not tolerate an unfamiliar clinical environment
Behavioural and communication difficulties act as significant barriers to these children accessing hospital care.
Children with autism and intellectual disability (ID) have a higher incidence of behavioural problems compared with children who have ID without autism
Behavioural concerns can include meltdowns, self-injurious behaviour and aggression.
This may indicate an underlying physical illness causing pain, emotional dysregulation, anxiety or communication difficulty, perhaps in relation to intolerance of change.
The underlying cause should be investigated
Children and teenagers with ASD, ID and other developmental disabilities have the same rights of access to health care and should be treated with the same dignity, respect and understanding shown to typically developing patients
Autistic children may exhibit:
- Impaired social communication and interaction
- deficits in social-emotional reciprocity
- decreased non-verbal communication
- Consider speaking in short sentences
- using fact-based, rather than feeling-based communication
- Restrictive, repetitive patterns of behaviour, interests or activities
- Stereotypies
- highly fixated routines
- inability to cope with sudden changes to routine.
- Routines enable young people with developmental disabilities to manage their internal states of distress.
- Similarly, changes in routine (eg acute or planned hospitalisation) can cause significant stress and distress
- Sensory sensitivities
- to loud or unexpected sounds, light, colours, textures, smells and/or touch
- may be hyper-sensitive or hypo-sensitive to these stimuli
- may trigger agitation but knowledge of these sensitivities may allow preventative measures to be put in place.
Presents differently at different stages of life
- infants and pre-schoolers
- unusual or delayed pattern of communication
- limited ability to interact or engage in play with others.
- slow to learn to speak or use words in an unusual way.
- rely less on nonverbal ways of communicating, such as eye contact, pointing and gestures.
- Carers may notice particular habits in play such as
- repeating the same action
- body movement
- exploring unusual aspects of toys.
- Some children need a strict routine in order to feel comfortable. Others develop a special interest that dominates their play.
- show unusual sensitivity or lack of sensitivity to sounds, textures, pain or light.
- They may start to become fussy about food.
- Children
- Present with difficulties in primary school.
- They may be good at communicating their needs and ideas
- but struggle to share information or join in conversations.
- They may prefer to follow their own ideas in play rather than take up the ideas of others.
- Many children have an intense special interest or series of special interests.
- Changing from one activity to another and dealing with unexpected changes can be harder for children with ASD.
- Heightened sensory sensitivity can lead to discomfort in classrooms or noisy environments.
- Children may fall behind academically and find it difficult to be part of social groups such as sports or clubs.
- Adolescence/adulthood
- may have a history of difficulty making lasting friendships
- experience high anxiety and have a very strong focus on particular ideas or interests
- appears to have extra support needs
- Girls with ASD are more likely to present later.
There are a range of conditions that may occur alongside ASD. They include:
- Attention Deficit Hyperactivity Disorder (ADHD)
- Global Developmental Delay
- Intellectual Disability
- Anxiety and mood disorders
- Challenging behaviour
- Learning difficulties
- Motor co-ordination difficulties
- Eating and sleeping difficulties.
- Medical and genetic disorders such as Fragile X Syndrome
Assessment
-
- History
- Is there anything immediate we can do to help your child?
- What was your child’s last visit like?
- How can we make this visit easier for you and your child?
- How would we know if your child is in pain?
- How can we best comfort your child?
- How does your child express their needs/desires?
- How does your child say yes/no?
- How does your child generally comprehend communication – verbal/non-verbal/visual?
- What would help us communicate with your child?
- What type of toys or activities does your child prefer?
- Does your child have difficulty with transitions? If so, what tends to help?
- Has your child had previous procedures? If so, which techniques were helpful or not helpful?
- Does your child respond to visual cues? Would a video or picture example of a procedure help?
- Acute presentation
- Determine if this has occurred previously, and how it was managed
- communication tools/aides
- behaviour management plans
- sensory considerations
- What has worked in the past
- Identify any potential triggers for the acute distress
- Is the child otherwise well? Check their observations
- Consider underlying pain. How does the child respond to pain whilst being examined?
- Consider changes to diet
- Assess fluid balance
- Look for potential sources of infection
- Consider changes in bowel habit, particularly constipation
- Examination
- It is important to look for the cause of an acute episode of distress or agitation. Consider pain or underlying physical illness as possible contributors
- This cohort of children may have higher pain thresholds
- Examine opportunistically
- A careful assessment is required.
- Examine and re-examine again until a cause is identified
- Communicate with the child before each step of the exam
- It is important to look for the cause of an acute episode of distress or agitation. Consider pain or underlying physical illness as possible contributors
- Determine if this has occurred previously, and how it was managed
- History
Management
- Investigations
- Consider basic investigations to look for a medical cause of an acute presentation, as indicated based on history and examination
- Aim to minimise distress by performing all relevant investigations together
Support for children with ASD
Following assessment, the next step is to develop a plan for supporting a child’s development, so as to enhance their existing skills and help them develop strategies to overcome difficulties.
Regular reviews by a paediatrician can help carers determine what is working and what else can be offered to their child.
In children under 7 years of age, an application to the National Disability Insurance Scheme (NDIS) can be made as soon as a child is found to have difficulties in two or more areas of development.
A child can receive services with this funding before having a formal diagnosis.
In children over 7 years, there is a need to meet access requirements to obtain NDIS funding.
A diagnostic report can help with eligibility.
There are also private services and community-based services that may be appropriate
Supportive Mx
- Crisis plan
- Everyday plan
- Community involvement
- School Mx strategy
- Parental & family education
MDT
- Psychology: to help manage emotions and challenging behaviours and develop social understanding
- Speech Pathology: to develop good communication skills and explore how language can be used for social engagement
- Occupational Therapy: to help determine the pattern of sensory responses for a child and how the environment should be changed to help a child. They also work with children to develop joint play skills.
Physio
Medication
- Medication is not recommended for the core features of ASD, but may be useful if a child had one of the co-occurring conditions listed above.
- Stimulants – help concentration / attention
- SSRIs – help with anxiety & depression
- Risperidone (+ atypical antipsychotics)
Acute behavioural disturbance management
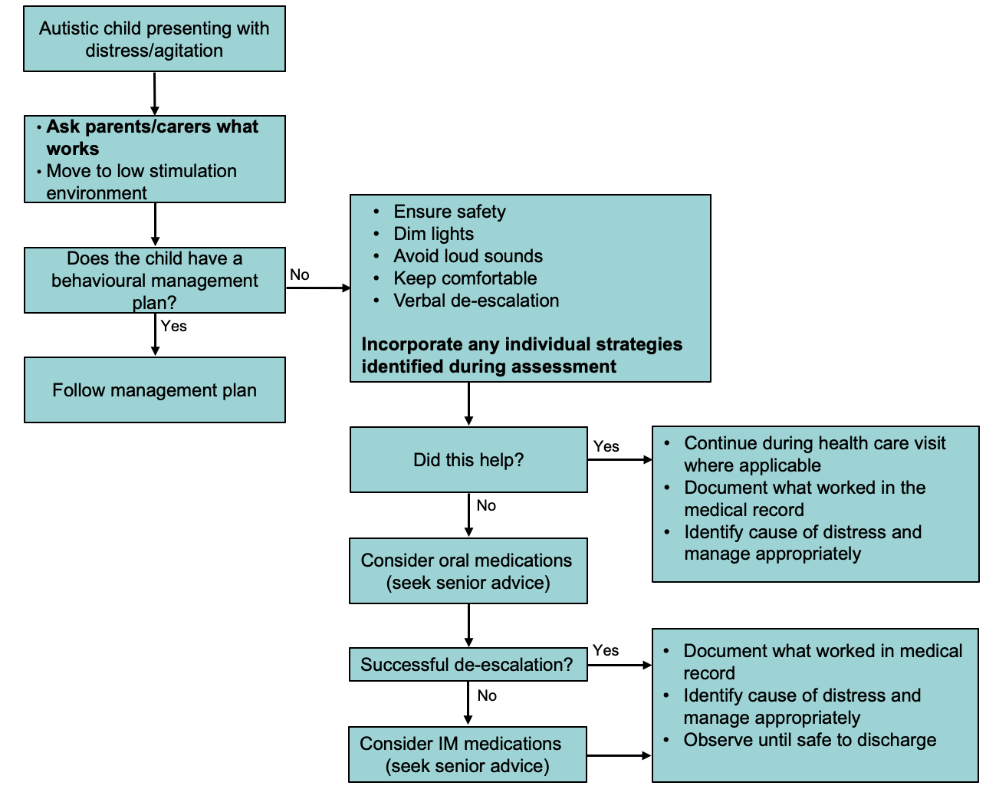
- Environmental modification
- Maintain a low stimulus environment, with dim lighting and minimise loud sounds
- Ensure familiar faces (parents or carers) are close by
- Minimise the number of staff entering the patient’s environment
- Attempt to make the environment as familiar to the child as possible, with the child’s own toys, bed sheets and pillows, if possible
- Use music and technology that the child is familiar with, if these are helpful
- Use appropriate sensory toys to distract the child
- Plan ahead for procedures
- Use Child Life (Play) Therapy techniques and staff early
- Explain any procedures to the child, in a form they can understand (eg use visual cards, photos, sign, gesture or simple instructions)
- Demonstrate what you are doing on a parent or carer (eg auscultation, using thermometer)
- Aim to minimise intervention, with all necessary investigations performed in the same procedure or under the same sedation, if required
- Have the child sit with their parent or carer for the procedure, if practicable
- Use distraction techniques
- Where possible, remove the IV cannula whilst the child is sedated to minimise distress caused by removing it later
- Psychotropic medication
- can be used in the non-acute pre-emptive management of agitation or anxiety during hospital visits or before procedures
- When considering the type of medication consider the following:
- Child’s current medications (with specific attention to drug-drug interactions)
- Contraindications in the medical and behavioural history, and individual-specific challenges
- Specific procedure/visit considerations (eg invasiveness, duration)
- See Acute behavioural disturbance: Acute management flowchart
- Once distress is managed, ensure to look for an underlying cause. If no medical cause is identified and there are ongoing concerns, consider a mental health referral

Medication Adverse Effects
|
Side-effect |
Medication association |
Management |
|
Respiratory depression |
Common with benzodiazepines, but also olanzapine or rapid administration of ketamine Droperidol can potentiate respiratory depression if used with opioids or other sedative medications |
Reversible with flumazenil if caused by benzodiazepines |
|
Extrapyramidal reactions |
Common with droperidol but can be seen with olanzapine, risperidone and quetiapine |
Reversible with benzatropine |
|
Neuroleptic Malignant Syndrome |
Seen with antipsychotics |
MET/ICU Check for elevated CK |
|
Paradoxical reactions |
Can be seen particularly in children with autism, developmental delay or history of escalating behaviour – benzodiazepines can result in increased agitation and anxiety |
2 Comments
Poh Chai
A lot of diagrams have broken link
asking if possible to reset it to make it visible
Morgoth
thank you for the message. I am working on it to improve it. will take some time