Colic (infantile)
- Key points
- Crying is normal physiological behaviour in young infants
- With typical history and normal examination, no investigations are required
- Parental education and close follow-up are vital to managing the unsettled or crying infant
- Excessive crying is associated with higher rates of parental post-natal depression
- Background
- At 6–8 weeks age, a baby cries on average 2-3 hours per 24 hours.
- “Colic” is an out-dated term used to describe excessive crying.
- The parents are often distressed, exhausted, and confused and often have received conflicting advice.
- Assessment
- Clinical characteristics of normal crying
- Increases in the early weeks of life and peaks around 6-8 weeks of age and usually improves by 3-4 months of age
- Usually worse in late afternoon or evening but may occur at any time
- May last several hours
- Infant may draw up legs as if in pain, but there is no good evidence that this is due to intestinal problems
- Red flags
- Sudden onset of irritability and crying
- Parental post-natal depression (PND) may be a factor in presentation
- Excessive crying is a strong risk factor for abusive head trauma (previously known as shaken baby syndrome)
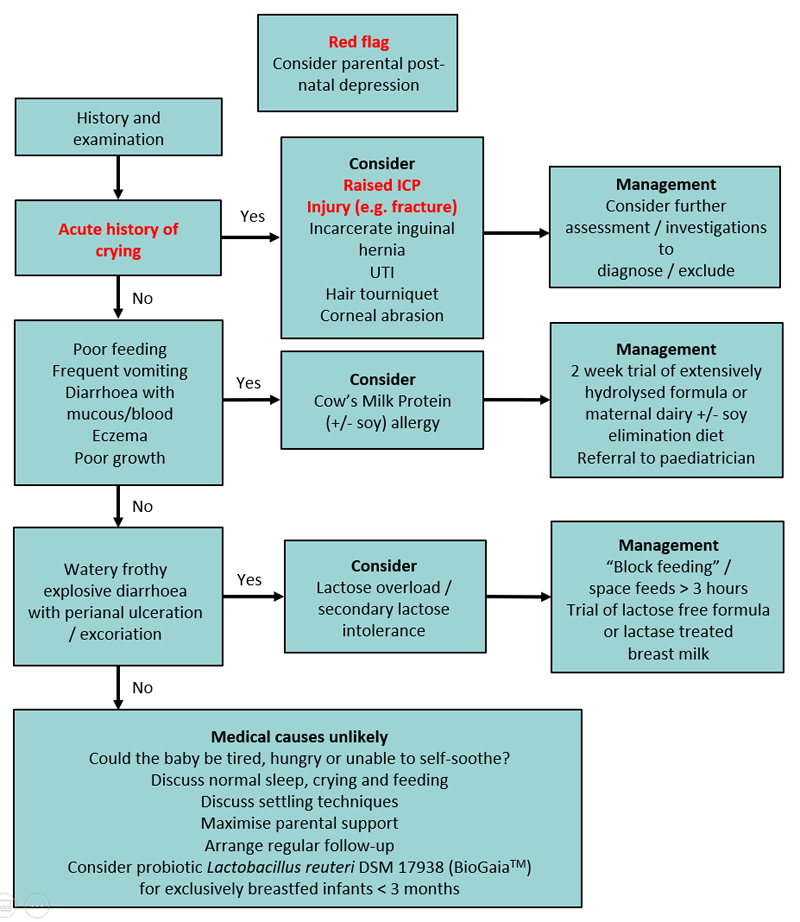
- Consider if crying is acute onset
- Raised intracranial pressure (ICP)
- Injury eg clavicle fracture, non-accidental injury
- Incarcerated inguinal hernia
- Urinary tract infection
- Hair tourniquet
- Corneal foreign body/abrasion
- Clinical characteristics of normal crying
- Common non-pathological causes of crying
- Excessive tiredness — consider if the infant’s total sleep duration per 24 hours falls more than an hour short of the “average” for their age
- Average sleep requirements:
- at birth: 16 hours
- at 2–3 months: 15 hours
- a 6 week old baby generally becomes tired after being awake for 1.5 hours
- a 3 month old baby generally becomes tired after being awake for 2 hours
- Hunger — more likely if there is poor weight gain
- Average sleep requirements:
- Excessive tiredness — consider if the infant’s total sleep duration per 24 hours falls more than an hour short of the “average” for their age
Differential diagnoses to consider
-
- Non-IgE cow milk / soy protein allergy
- Both can be found in human breast milk if in the mother’s diet
- Goat milk protein is as allergenic as cow milk protein
- Suspect if there is:
- significant feeding problems that persist day and night
- frequent vomiting
- diarrhoea with blood or mucus
- poor weight gain
- wide-spread eczema
- Clinical diagnosis by trialing eliminating cow / soy milk for 2 weeks:
- modifying the mother’s diet
- or changing to an extensively hydrolysed formula (requires paediatrician consultation)
- and requires resolution of symptoms or re-emergence of symptoms on rechallenge
- Lactose overload / malabsorption
- Consider lactose overload if infant has very frequent breastfeeds and frothy, watery diarrhoea with perianal excoriation
- Primary lactose intolerance is extremely rare
- Gastro-oesophageal reflux disease (GORD)
- No causal relationship between gastro-oesophageal reflux (GOR) and infant crying and irritability has been demonstrated
- Gastro-oesophageal reflux disease is rare
- Proton pump inhibitors have been shown to be ineffective in reducing crying
- Non-IgE cow milk / soy protein allergy
Acute management
Investigations
- If the history is typical and examination normal, no investigations are required
Management
- Exclude medical cause
- Parental education and reassurance. It is often helpful to explain to caregivers the potential causes of crying that have been excluded and the reasons for excluding each condition
- Assess parental emotional state and mother-baby relationship:
- invite the parent/s to talk about how stressful it is to care for a baby who cries persistently
- ascertain whether the parent is worried that she/he is depressed
- screen for postnatal depression using the Edinburgh Postnatal Depression Scale
Parental Education
- Most importantly, listen to parents and validate their concerns.
- If you have an infant who is happily vomiting and is growing well, provide reassurance to parents that their baby is physically healthy and a ‘happy chucker’.
- For infants who are crying and irritable
- discuss normal sleep and crying patterns (PURPLE Crying Curve, below)
- baby could be ‘physically healthy, but a high crier’; and settling techniques
- Engage in a partnership with the parent/s
- This includes acknowledging their concerns
- taking time to observe the baby-parent interactions and offering follow-up
- Observing the baby feed is helpful for parents who are concerned about their baby’s feeding
- Explain normal crying and sleep patterns
- Use the normal crying curve to explain the natural history of infant crying (taken from Purple Crying – see parent information below)
- Use a sleep/cry diary to explain the infant’s cry/sleep/feeding patterns
- Encourage parents to recognise signs of tiredness (frowning, clenched hands, jerking arms or legs, crying, grizzling)

- Assist parents to help their baby deal with discomfort and distress
- Establish pattern to feeding/settling/sleep
- Aim to settle the baby for daytime naps and night-time sleep in a predictable way (eg, quiet play, move to the bedroom, wrap the baby, give the baby a brief cuddle, then settle in the cot while still awake)
- Avoid excessive stimulation – noise, light, handling. Excessive quiet should also be avoided. Most babies find a low level of background noise soothing.
- Darken the bedroom for daytime sleeps
- Carry baby in a papoose in front of the chest
- Baby massage/rocking/patting
- Gentle music
- Respond before baby is too worked up
- Give the primary carer permission to rest once a day without the need to carry out household chores. Have somebody else care for the baby for brief periods to give the parent/s a break
- Provide printed information as parents are unlikely to remember much given their state of mind at the time
- Medications and other treatment options
- Medication is not indicated, this includes:
- Anti-reflux medications — ineffective in reducing crying compared with placebo
- Anticholinergic medications — due to risk of serious adverse events eg apnoeas, seizures
- Colic mixtures (eg gripe water) – no proven benefit
- Simethicone (eg Infacol™) – no effect on crying compared with placebo
- There is limited evidence to support probiotic use
- Only in exclusively breastfed infants under 3 months, the probiotic Lactobacillus reuteri DSM17938 (BioGaia™) has been shown to be effective with excessive crying (colic)
- To be given as 5 drops per day orally to the infant for 21 days only
- It should not be given to formula-fed infants
- The probiotic has not been shown to be effective in both breastfed and formula-fed infants in Victoria, Australia
- Probiotic effects are strain-specific; Lactobacillus reuteri DSM17938 is the only probiotic strain with some evidence of efficacy in exclusively breastfed infants with excessive crying (colic)
- Formula changes are usually not helpful unless there is proven cow milk allergy. Weaning from breast milk has no benefit
- Spinal manipulation is not indicated and has associated risks
- Medication is not indicated, this includes:
- Consider consultation with local paediatric team when
- Medical cause of crying identified or suspected
- Baby clinically unwell
- Admission to hospital — if infant considered at risk of non-accidental injury or parental exhaustion