Neck MASSES in KIDS
divided into the broad categories of congenital, inflammatory/infective and neoplastic
| Paediatric cervical masses according to anatomical location | |||
| Location | Aetiology | ||
| Congenital | Inflammatory/infective | Neoplastic | |
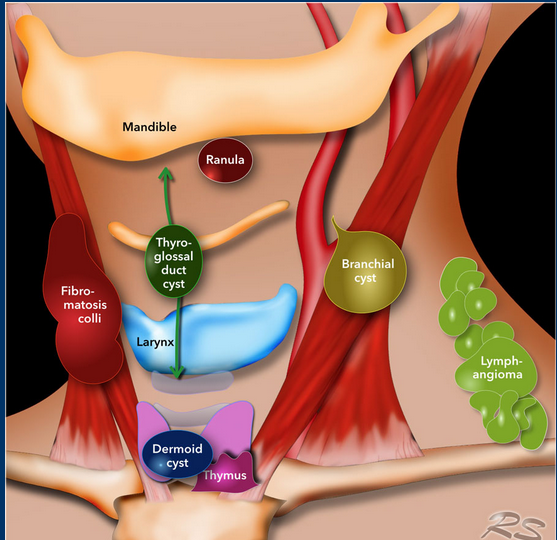
| Submental | Thyroglossal cyst Dermoid cyst | Sialadenitis Lymphadenitis Reactive lymphadenopathy | Malignant lymphadenopathy Benign connective tissue tumour |
| Submandibular | Vascular or lymphatic malformation Branchial cleft cyst | Sialadenitis Lymphadenitis Reactive lymphadenopathy | Malignant lymphadenopathy Salivary gland tumour Benign connective tissue tumour |
| Carotid triangle | Vascular or lymphatic malformation Branchial cleft cyst | Lymphadenitis Reactive lymphadenopathy Sternocleidomastoid tumour of infancy | Malignant lymphadenopathy Benign connective tissue tumour |
| Muscular triangle | Thyroglossal duct cyst Dermoid cyst | Goitre | Thyroid tumour Benign connective tissue tumour |
| Posterior triangle | Vascular or lymphatic malformation | Lymphadenitis Reactive lymphadenopathy | Malignant lymphadenopathy Benign connective tissue tumour |
| Comparison of common benign and red flag conditions | |||
| Condition | Pathophysiology | Clinical features | Management |
Thyroglossal duct cysts | Congenital abnormality that may present at any age, though typically diagnosed prior to adulthood Occurs as a result of failure of the thyroglossal duct to involute | Most common midline congenital neck mass Arises anywhere along the midline path of the thyroglossal duct Suspect if ongoing midline mass following resolution of infection | If asymptomatic, can be managed conservatively Treatment involves surgical excision (Sistrunk’s procedure) |
Branchial cleft abnormality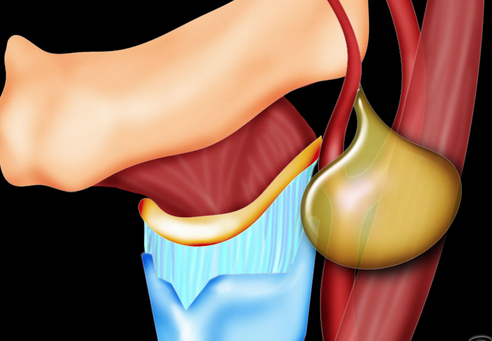 | Congenital abnormality that may present at any age, though typically diagnosed prior to adulthood Occurs as a result of failure of the pharyngeal clefts to involute | Most common lateral congenital neck mass May present as a cyst, sinus or fistula that can become infected Can arise in numerous positions in the head and neck, most typically in the anterolateral neck | If asymptomatic, can be managed conservatively Treatment involves surgical excision |
| Reactive lymphadenopathy | Occurs secondary to a local infective or inflammatory process May be complicated by secondary infection | Most common cause for paediatric neck mass Presents with transiently enlarged, tender lymph nodes May occur at any age, though most commonly seen in infancy | Expectant management appropriate for up to six weeks Empiric antibiotics may be used if bacterial infection is suspected |
| Lymphoma | Diffuse group of malignant tumours of lymphoid tissue Hodgkin’s lymphoma is differentiated by the presence of Reed-Sternberg cells | Most common cause for malignant paediatric neck mass Rare in children younger than five years Hodgkin’s lymphoma presents with cervical adenopathy more commonly than non-Hodgkin’s lymphoma | Depending on the cell subtype, treatment involves chemotherapy or radiotherapy |
| Rhabdomyosarcoma | Thought to arise from primitive striated muscle cellsMost cases are sporadic, though an association with neurofibromatosis and Li Fraumeni syndrome exists | Incidence peaks at age 2–5 years and 15–19 yearsMost common soft tissue malignancy in children Up to 89% of cases present in the nec | Management may involve a combination of surgery, radiotherapy and chemotharpy |

- Timeline
- Neonatal and early infancy are usually congenital
- Include teratomas, sternocleidomastoid tumors, vascular or lymphatic malformations
- Vascular and lymphatic malformation present at birth and grow with the child
- Reactive lymphadenopathy common infancy and early childhood
- Congenital masses may present later because of continued grow or superimposed infection
- Likelihood of malignancy increases with later childhood/ adolescence
- Neonatal and early infancy are usually congenital
- Time course
- Rapid – usually inflammatory/ infectious, including secondary infection of an underlying mass
- Inflammation usually resolves in 6 weeks
- Cervical mass > 6 weeks – further evaluate
- If potentially effecting airway or contain abscess – refer
- Associated symptoms
- Viral prodrome, fevers, tenderness – reactive lymphadenopathy, consider suppurative lymphadenitis or infection underlying mass
- Malignant neck masses typically asymptomatic – consider B symptoms, anemia, thrombocytopenia
- Red flag features of presentation
- Weight loss
- Sustained fevers/night sweats
- Generalised lymphadenopathy
- Signs and symptoms of pancytopenia
- Mass persisting >6 weeks
- Lymph node >3 cm
- Thyroid mass
- Supraclavicular mass
- Hard, irregular mass
- Fixed mass
- Risk factors
- URTis, cat scratch, mycobacterial infection – animals, overseas, tick bites
- Hx of radiation, family history of malignancy
- Location
- Midline – more likely congenital
- Thyroglossal duct cyst – anywhere along embryological pathway from base of tongue to thyroid gland. Often at hyoid bone. Will elevate with tongue protrusion or swallowing
- Dermoid cysts tethered to overlying skin
- Thyroid masses – need further evaluation
- Midline – more likely congenital
- Palpation
- Reactive lymphadenitis – collection small, tender mobile lumps
- Consider suppurative – warmth, fluctuance, induration, severe tenderness
- Malignancy – firm, irregular, immobile or fixed
- Size
- Cervical node < 1cm can be normal in children
- Examine ENT and for stigmata hematological malignancy
- Investigations
- FBC, blood film
- Targeted serolgical investigation for atypical infection
- USS, consider referral for FNA (often need anaesthetic)
- do CT or MRI if strong suspicion Ca
- Investigations for atypical infection in lymphadenopathy
- TB testing
- Epstein-Barr virus titre
- Cytomegalovirus titre
- Human immunodeficiency virus titre
- Toxoplasmosis titre
- Management
- Watchful waiting 6 weeks for suspected lymphadenitis – bilateral, no red flag features
- 10 days Augmetnin/cephalexin/clindamycin for suspected suppurative lymphadenitis – if not improving 4 weeks – investigate/refer sooner if deteriorating
- All neck masses suspicious for non-haematological malignancy (Red Flags above) are best referred urgently to a head and neck surgeon for further evaluation including possible biopsy.
- Medical imaging, including USS, CT or MRI, may be considered as part of the referral