Anorexia
- Restriction of energy intake relative to requirements 🡪
- leading to a significantly low body weight in the context of age, sex, developmental trajectory, and physical health.
- Significantly low weight is defined as a weight that is less than minimally normal or, for children and adolescents, less than minimally expected.
- leading to a significantly low body weight in the context of age, sex, developmental trajectory, and physical health.
- even though at a significantly low weight:
- Intense fear of gaining weight or of becoming fat, or
- persistent behaviour that interferes with weight gain
- persistent lack of recognition of the seriousness of the current low body weight.
Specify whether:
Restricting type:
- weight loss is accomplished primarily through dieting, fasting and/or excessive exercise.
- During the last three months has not engaged in recurrent episodes of binge eating or purging behaviour (i.e. self-induced vomiting, or the misuse of laxatives, diuretics, or enemas).
Binge-eating/purging type:
- During the last three months the individual has engaged in recurrent episodes of binge eating or purging behaviour (i.e. self-induced vomiting, or the misuse of laxatives, diuretics, or enemas).
- Female
- 13–25 years
- BMI <18.5 (note that BMI less useful in adolescents)
Specify current severity:
- Mild: BMI more than 17
- Moderate: BMI 16- 16.99
- Severe: BMI 15-15.99
- Extreme: BMI less than 15
Assessment:
- History
- Assess risk of suicide
- SCOFF questionnaire:
- Do you make yourself Sick because you feel uncomfortably full
- Do you worry that you have lost Control over how much you eat
- Have you recently lost more than One stone (6.35 kg) in a 3-month period?
- Do you believe yourself to be Fat when others say you are too thin?
- Would you say Food dominates your life?
- If the patients answer ‘Yes’ to 2 or more then there is a high index of suspicion that they have an eating disorder and warrant a more detailed assessment
- Once there is an index of suspicion a systematic approach to the medical assessment is required to:
- Determine the severity of malnutrition
- Screen for other causes of weight loss
- Establish who delivers treatment and the setting of care
Examination
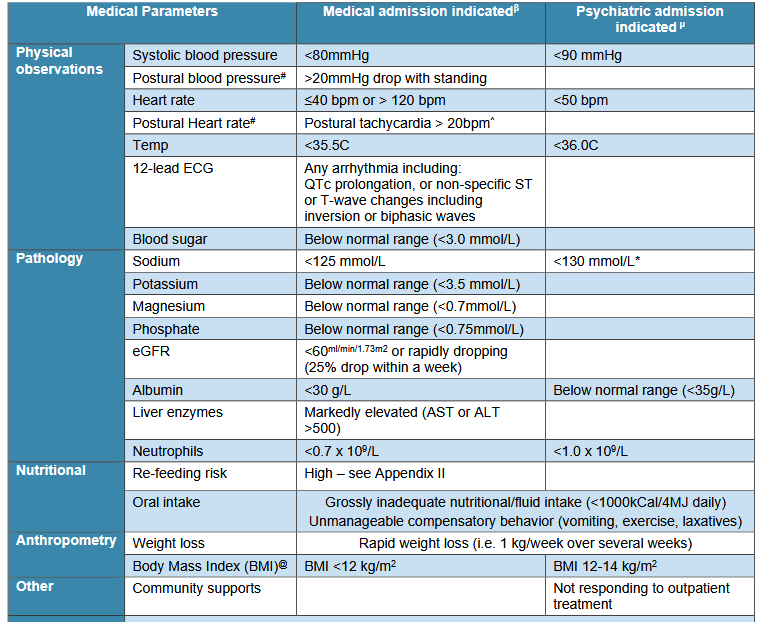
Alert parameters include:
- BMI <14
- Systolic BP <90 mm
- HR ≤40 or >120 bpm
- Significant postural tachycardia or BP changes
- Electrolyte abnormalities
- Non-responsiveness to community treatment
- Rapid weight loss
- Grossly inadequate nutritional intake
- Anaemia, dry skin, dry hair, lanugo
- Dental caries, parotid enlargement
- Ix Alert parameters include:
- WCC < 2
- Hb < 90
- K+ < 3
- Na+ < 130
- Albumin < 32
- CK > 250
Management
- Usual practice is community based management with referral to dietician/ psychiatrist/ psychologist/ local MHS/ specialist program and ongoing GP FU
- Recovery can take many years
- No evidence for antidepressants for AN symptoms
- SSRIs beneficial for comorbid anxiety and depression
- A patient with anorexia nervosa can be kept alive by enforced treatment but it is difficult for them to enter into any meaningful recovery until they are willing to engage with biological and psychological treatment
- Hospitalization should also be considered for:
- If ONE or MORE of these parameters is met at the time of assessment, inpatient treatment is advised
- Immediate danger to life from physical deterioration
- Suicide risk
- No adequate outpatient option
Once DISCHARGED
- Education by dietitian for patient plus family/carers re: discharge meal plan
- CBT:
- body perception
- coping mechanisms
- sets clear weight goals and expectations
- makes use of recording sheets
- targets maintaining factors such as negative body image
- family-based treatment
- is primarily used in the paediatric system
- main focus is on weight restoration andreturn to physical health
- Established community treatment plan including:
- GP review for ongoing medical monitoring at least weekly or more frequently dependent on clinical indications. MONITOR
- weight, bloods
- physical observations (postural measures of both BP & HR)
- ecg
- postural BP
- Community dietitian if available
- Psychosocial support – If the patient is willing, evidence-based psychological treatment (e.g. CBT-e, SSCM, or Day Program delivered by a clinician experienced in treatment of eating disorders) and Referral of carers to appropriate support services for skills training to identify risk, encouraging help seeking and treatment engagement, and sustaining a recovery focus.
- A GP care plan
- Better Access Mental Health Care Plan
- Chronic Disease Management Plan
- Eating Disorder Treatment and Management Plan
- Established early intervention plan (e.g. identified readmission criteria) developed in collaboration with family/community supports to facilitate voluntary solution focussed admissions as appropriate
- GP review for ongoing medical monitoring at least weekly or more frequently dependent on clinical indications. MONITOR
Prognosis
- adolescent onset has much better prognosis than adult onset)
- only about 50% make a full recovery
- with treatment, 70% resume a weight of at least 85% of expected levels and about 50% resume normal menstrual function
- eating peculiarities and associated psychiatric symptoms are common and persistent
- high rates of mortality (7%) secondary to severe and chronic starvation, metabolic or cardiac catastrophes, with a significant proportion dying by suicide