Bulimia Nervosa
- Recurrent episodes of binge eating. An episode of binge eating is characterized by both:
- Eating in a discrete period of time (e.g. within any 2 hour period), an amount of food that is definitely larger than what most individuals would eat in a similar period of time under similar circumstances;
- A sense of lack of control over eating during the episodes (e.g. a feeling that one cannot stop eating or control what or how much one is eating.
- Recurrent inappropriate compensatory behaviors to prevent weight gain, such as
- self-induced vomiting
- misuse of laxatives
- diuretics, or other medications
- fasting
- excessive exercise.
- The binge eating and inappropriate compensatory behaviors both occur, on average, at least once a week for 3 months.
- Self-evaluation is unduly influenced by body shape and weight.
- The disturbance does not occur exclusively during episodes of anorexia nervosa.
- Specify current severity:
- Mild: An average of 1-3 episodes of inappropriate compensatory behaviours per week.
- Moderate: An average of 4-7 episodes of inappropriate compensatory behaviours per week.
- Severe: An average of 8-13 episodes of inappropriate compensatory behaviours per week.
- Extreme: An average of 14 or more episodes of inappropriate compensatory behaviours per week.
Associated Features
- fatigue and muscle weakness due to repetitive vomiting and fluid/electrolyte imbalance
- tooth decay, perioral irritation, mouth ulcers
- swollen appearance around angle of jaw and puffiness of eye sockets due to fluid retention, edema
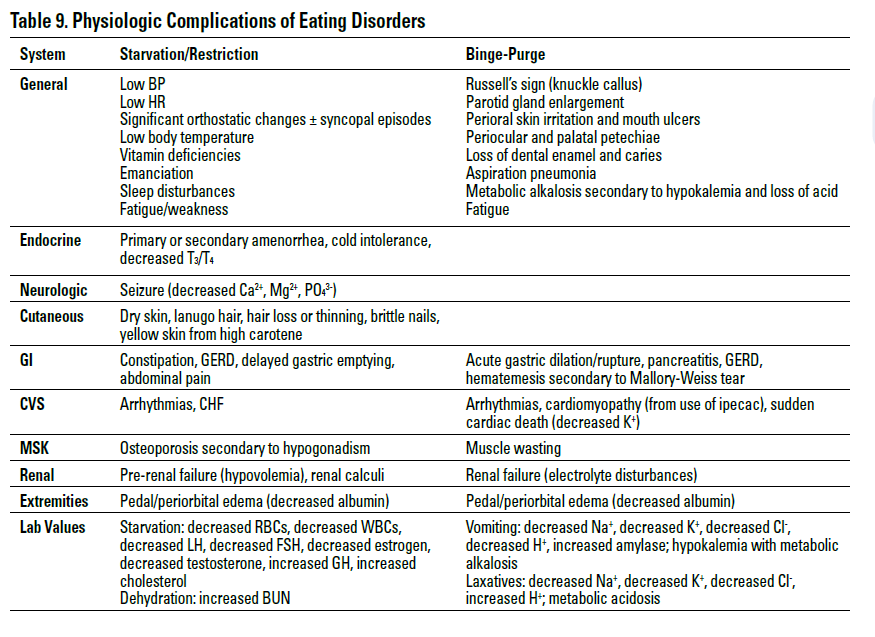
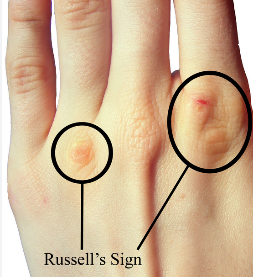
- reddened knuckles, Russell’s sign (knuckle callus from self-induced vomiting)
- trouble concentrating, fatigue, headache, abdominal pain/reflux
- weight fluctuation over time
Management
- medical admission for significant electrolyte abnormalities
- biological: treatment of starvation effects, SSRIs (60 mg fluoxetine has the most evidence) as adjunct
- psychological: develop trusting relationship with therapist to explore personal etiology and triggers, CBT, family therapy, recognition of health risks
- Encourage excellent and healthy eating
- Recognize hunger, eat healthy food.
- Encourage others to do the same rather than stay hungry.
- Eat a variety of food and make all kinds of the food part of your diet to keep it balanced.
- Develop a taste for everything, and enjoy the meal.
- Discourage and avoid making comments on food and promote eating healthy food.
- Educate about damages associated with poor eating patterns and eating disorders.
- Encourage excellent and healthy eating
- social: challenge destructive societal views of women, use of hospital environment to provide external patterning for normative eating behaviour
Prognosis
- relapsing/remitting disease
- good prognostic factors: onset before age 15, achieving a healthy weight within 2 yr of treatment
- poor prognostic factors: later age of onset, previous hospitalizations, individual and familial disturbance
- 60% good treatment outcome, 30% intermediate outcome, 10% poor outcome (mortality rate of approximately 2% per decade)