Major Depressive Disorder (MDD)
EPIDEMIOLOGY
- common with lifetime prevalence of 15% & up to 25% for women
- Incidence is 10% of 1° care pts & 15% of medical inpatients
- F:M 🡺 MDD is 2x more common in women (hormones, childbirth, ψ-social stressors, learned helplessness)
- Average age of onset is 40yo, 50% have 1st episode between 20-50yo
- More common in people without close interpersonal relationships (divorced/separated)
Prognosis
- can appear at any age
- increases with the onset of puberty.
- onset peaks in the mid-20s
- The course of MDD
- some individuals have a chronic illness course
- some have years with few or no symptoms between depressive episodes
- 50% of depressive episodes are brief and resolve within three months
- Risk of recurrence
- 1 ep → 50%
- 2 eps → 70%
- 3 eps → 90%
- factors for chronic symptoms or recurrence
- early age of onset
- greater number of episodes
- severity of the initial episode
- disruption of the sleep-wake cycle
- presence of comorbid psychopathology (particularly dysthymia)
- a family history of psychiatric illness
- presence of negative cognitions
- high neuroticism
- poor social support
- stressful life events
- underlying personality
- underlying substance use disorders
having a longer duration of depression before initiation of Tx
→ these pts may benefit from long-term antidepressant Tx
- The longer the period of full remission, the lower the chance of recurrence.
- Negative prognostic factors
- psychotic features
- comorbid anxiety
- personality disorders
- greater symptom severity.
- good prognostic factors:
- solid friendships during adolescence
- stable family
- social functioning
- absence of comorbid ψ disorder or personality disorder
- late age of onset
- Many individuals with bipolar disorders are initially misdiagnosed with a major depressive disorder, but over the course of the illness, will later be correctly diagnosed with bipolar disorder.
- This is especially true for individuals who present with mixed features (i.e. – some symptoms of bipolar, but not full hypomanic or manic episodes).
- The impairment from MDD can range from being mild to severe, depending on the individual, and depend on the symptom profile
- Severity Specifier
- Mild:
- Few, if any, symptoms in excess of those required to make the diagnosis are present, the intensity of the symptoms is distressing but manageable, and the symptoms result in minor impairment in social or occupational functioning.
- Moderate:
- The number of symptoms, intensity of symptoms, and/or functional impairment are between those specified for “mild” and “severe.”
- Severe:
- The number of symptoms is substantially in excess of that required to make the diagnosis, the intensity of the symptoms is seriously distressing and unmanageable, and the symptoms markedly interfere with social and occupational functioning.
- Mild:
- Remission Specifier
- Severity Specifier
- In partial remission:
- Symptoms of the immediately previous major depressive episode are present, but full criteria are not met, or there is a period lasting less than 2 months without any significant symptoms of a major depressive episode following the end of such an episode.
- In full remission:
- During the past 2 months, no significant signs or symptoms of the disturbance were present.
Risk factors
- Family Hx of depression
- Hx of
- prepubertal trauma
- neglect
- loss of a parent
- sexual, physical or emotional abuse
- life stresses:
- bereavement
- redundancy
- stressful living environment
- Medications
- Antihypertensives: beta-blockers & calcium channel blockers
- Glucocorticoids
- Antimicrobials
- Systemic analgesics
- Antiparkinsonian meds
- Anticonvulsants
DSM-IV-TR for Major Depressive Episode (SADAFACES)
- at least 5/9 of the following with at least 1 being either anhedonia or depressed mood
- nearly every day for at least 2/52 & represent a change from pre-morbid functioning
- does NOT include Sx due to
- general medical condition or
- mood-incongruent delusions/hallucinations
S – sleep (insomnia esp. terminal or hypersomnia)
A – anhedonia (loss of interest/pleasure in all activities most of the day)
D – depressed mood most of the day, nearly every day (may be irritable mood in children/adolescents)
A – appetite ↓ & wt loss when not dieting or wt gain (Δ5% in 1/12)
F – fatigue or lack of energy
A – agitation or ψ-motor retardation
C – concentration ↓ or indecisiveness
E – excessive guilt (may be delusional)or feelings of worthlessness
S – suicidal ideation or recurrent thoughts of death
- Sx are not better accounted for by bereavement (loss of loved one & Sx for >2/12 with functional impairment, morbid preoccupation with worthlessness, suicidal ideation, psychotic Sx or ψ-motor retardation)
Symptoms
- Mood symptoms:
- Varies from mild sadness to intense feelings of guilt, worthlessness & hopelessness
- Abnormal irritable mood
- Talk: impoverished, slow & monotonous
- Cognitive symptoms
- Futility, guilt, self-reproach, unworthiness
- Anhedonia – devoid of pleasure
- Worrying
- Persecution
- Impaired learning
- Inability to concentrate
- Marked forgetfulness
- Ruminations
- Lack of decisiveness
- Pseudodementia in elderly pts
- With more severe disease:
- hypochondriacal preoccupations
- suicidal thoughts
- nihilism – delusion of the non-existence of the self or part of self; engagement in activities which are totally destructive to one’s own purposes or those of one’s group
- Physical/somatic complaints:
- Headache
- Sleep
- Early waking
- Disrupted – frequent waking throughout the night
- Reduced or excessive
- Change in appetite
- Constipation
- Loss of libido
- Erectile dysfunction
- Fatigue or loss of energy → lethargic
- Bodily aches & pains
- Weight loss – sign of more severe diseas
- Children are more likely to present with somatic symptoms, fears and phobias.
- Adolescents are more likely to be irritable and aggressive, with a tendency to withdraw rather than have an outward show of sadness
- Behaviour
- Psychomotor Agitation or retardation
- Restlessness or slowed so significantly as to be recognized by others
- Retardation or agitation
- Anxiety
- Poverty of movement & expressions
- Loss of interest, with diminished involvement in work & recreation
- Psychomotor Agitation or retardation
- Hallucinations
- Auditory – often hostile, critical
Differentials
- medical disorders (general medical condition)
- substance-induced
- mononucleosis (EBV)
- thyroid or adrenal dysfunction
- AIDS (neurotrophic virus – affinity for neural tissue)
- Medication (cardiac, anti-HTN, sedatives, hypnotics, anti-psychotics, anti-epileptics, anti-parkinsonian, analgesics, antibacterials & anti-neoplastic drugs)
- Neurological disorders
- Parkinson’s (50-75% have depression, motor Sx masked by PD – bradykinesia, resting tremor, rigidity, postural hypotension)
- Alzheimer’s
- Epilepsy (esp. temporal lobe epilepsy)
- Stroke
- Tumours
- Pseudodementia
- Cognitive Sx in MDD have sudden onset & diurnal variation (not present in 1° dementia), depressed pts do not try to answer questions (“I don’t know”) whereas pts with dementia try to confabulate.
- In MDD, recent memory is more affected than remote memory (sometimes can be coached into remembering – unlike demented pts).
- Bipolar I or II
- have to rule out if they have had mania-like Sx
- other mental disorders
- psychotic disorders, eating disorders, adjustment disorders, somatoform disorders & anxiety disorders all commonly associated with depressive Sx
- most difficult is DDx of “anxiety with depression” vs. “depression with marked anxiety”-
- Bereavement and Loss
- Responses to a significant loss (e.g. – bereavement, financial ruin, losses from a natural disaster, a serious medical illness or disability)
- feelings of intense sadness
- rumination about the loss
- insomnia
- poor appetite
- weight loss noted
- Although such symptoms may be understandable or considered appropriate to the loss, the presence of a major depressive episode in addition to the normal response to a significant loss should also be carefully considered. This decision inevitably requires the exercise of clinical judgment based on the individual’s history and the cultural norms for the expression of distress in the contest of loss
- Responses to a significant loss (e.g. – bereavement, financial ruin, losses from a natural disaster, a serious medical illness or disability)
| Presentation | Grief | Major Depressive Episode |
| Predominant affect | Emptiness, loss | Persistent low mood, inability to feel happiness or pleasure |
| Course | Decreases in intensity over days to weeks, and occurs in waves (“pangs of grief”) | Persistent and not tied to specific thoughts |
| Thought Content | Mostly preoccupied with thoughts and memories of the deceased | Self-critical, pessimistic ruminations |
| Self-esteem | Preserved* | Worthlessness, self-loathing is common |
| Death thoughts/suicidal ideation | Thoughts involve wanting to “join” the deceased | Idea of ending one’s life associated with feelings of worthlessness, pain of depression |
* = If self derogatory ideation is present in grief, it usually involves feelings with respect to the deceased (e.g. – not visiting frequently enough, not telling the deceased how much they were loved)
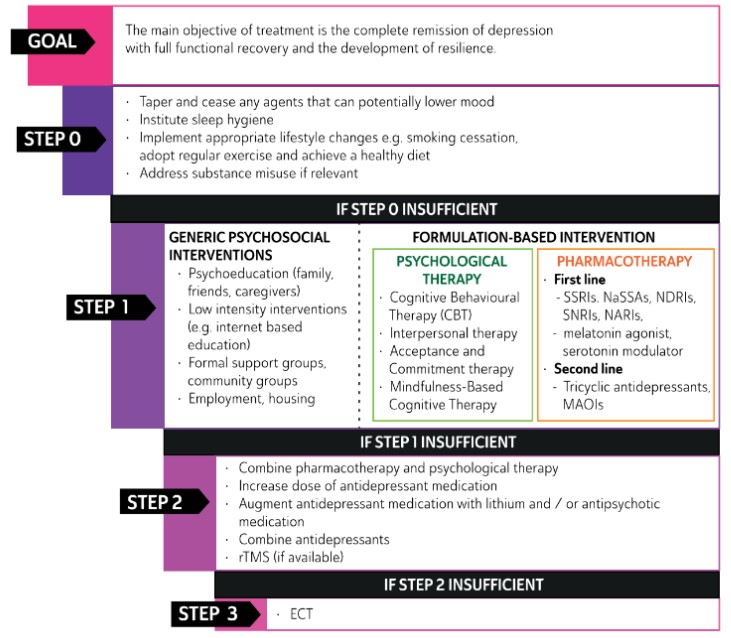
Management of Depression
- Safety (person, others including staff, children, elderly, etc)
- ? hospitalise or outpatient treatment (Mental Health Act 2000 criteria satisfied for involuntary assessment or treatment)
- Suicidality, homicidality, grossly reduced ability to get food/shelter, rapidly progressing Sx & breakdown of social supports, depression with psychotic features are compelling indications for hospitalisation
- Depressed & manic pts often lack insight
- Therapeutic alliance (build rapport, trust & stable relationship with pt)
- just talking to the patient & letting them tell their story can be very therapeutic
- may be the only adult relationship built on trust & support
- repetitive formation & subsequent break of therapeutic relationship (eg sessions once weekly) also help the pt understand that relationships are possible & encourages them to take ownership of their issues
- Diagnostic clarification (collateral Hx, physical examination, Ix, serial MSE)
- collateral Hx (family/friends, GP, landlord, hospital notes, etc)
- physical examination (hypo/hyperthyroid, neurological conditions, Cushing’s syndrome, iatrogenic)
- investigations (UDS, FBC, ELFTs, B12, folate, TFTs, ESR, Ca/Mag/Phos, imaging – CT head, CXR)
- serial MSE comparison
- Sx control (bio-ψ-social looking at short & long term goals)
- Competence & ability to consent, etc.
Pharmacological options: Anti-depressants
Antidepressant drugs are indicated for patients with:
- major depression (characterised by marked symptoms and functional impairment)
- melancholia (characterised by significant psychomotor symptoms – agitation or retardation)
- psychotic depression (depression with delusions or hallucinations).
- onset of effect
- relief of neuro-vegetative/physical symptoms: 1-3 wk
- relief of emotional/cognitive symptoms: 2-6 wk
- However any adverse effects of the drug can be experienced immediately.
- Thus a pt will often feel worse before they begin to feel any benefit from the medications→ prior to prescribing antidepressants, pts must be fully educated about this.
- Reducing dose
- Tapering usually required to avoid withdrawal reactions
- speed of taper is based on the medication’s half-life and the patient’s individual sensitivity
- fluoxetine does not require a taper due to its long half-life
- paroxetine and venlafaxine require a slower taper than sertraline or citalopram
The choice of medication is guided by:
- the severity of the pt’s illness
- adverse effects
- ease of use
- whether or not they respond to the drugs
- if there is a family Hx → consider trialling the drug that worked for the family member
- possibility of drug interactions → v impt to check pt’s existing medication list
categories:
- Tricyclic Antidepressants
- Amitriptyline (Elavil)
- Nortriptyline (Pamelor)
- Serotonin Norepinephrine Reuptake Inhibitors (SNRI)
- Venlafaxine (Effexor)
- Desvenlafaxine (Pristiq)
- Duloxetine (Cymbalta)
- Selective Serotonin Reuptake Inhibitors (SSRI)
- Paroxetine (Paxil)
- Fluoxetine (Prozac)
- Sertraline (Zoloft)
- Fluvoxamine (Luvox)
- Citalopram (Celexa)
- Escitalopram (Lexapro)
- Vortioxetine (Brintellix) – New since 2013, similar to generic SSRIs, with more Nausea at 10x the cost
- Norepinephrine Dopamine Reuptake Inhibitor (NDRI)
- Bupropion (Zyban)
- Norepinephrine Antagonist Serotonin Antagonist (NASA)
- Mirtazapine
- Selective norepinephrine reuptake inhibitors (NRIs)
- Reboxetine, atomoxetine
- melatonergic MT1 and MT2 receptors agonist and selective serotonergic 5-HT2B and 5-HT2C receptors antagonism (MASSA)
- Agomelatin
- Monoamine Oxidase Inhibitor (MAO Inhibitor)
Forest plots of network meta-analysis of all trials efficacy (A) and acceptability (B) Antidepressants were compared with placebo

Doses of most commonly used antidepressants | ||
| Initial Dose (mg) | Range (mg) | |
| SSRIs | ||
| Citalopram | 20 | 20–40* |
| escitalopram | 10 | 10–20** |
| fluoxetine | 20 | 20–80 |
| Paroxetine | 20 | 10–50 |
| Paroxetine extended release | 25 | 25–62.5 |
| sertraline | 50 | 50–200 |
| SNRIs | ||
| Duloxetine | 40–60 | 40–60 |
| Venlafaxine extended release | 37.5–75 | 75–225 |
| Desvenlafaxine | 50 | 50 |
| Atypical | ||
| Bupropion | 100 twice a day | 100–400*** |
| Bupropion extended release (Xl) | 150 | 150–450 |
| Mirtazapine | 37.5–75 | 15–45 |
| trazodone Contramid CoaD | 150 | 150–300 |
Symptoms and initial antidepressant choice
| Symptoms | Preferred antidepressant |
| Anxiety | Selective serotonin reuptake inhibitors Moclobemide |
| Weight loss, reduced appetite | Mirtazapine Mianserin |
| Sleep disturbance, insomnia | Agomelatine Mirtazapine Mianserin Tricyclic antidepressants |
| Sexual dysfunction | Agomelatine |
| Blunting, anhedonia, demotivation | Selective serotonin reuptake inhibitors Serotonin noradrenaline reuptake inhibitors Agomelatine Monoamine oxidase inhibitors Reboxetine |
| Melancholia, severe depression | Serotonin noradrenaline reuptake inhibitors Tricyclic antidepressants Vortioxetine Monoamine oxidase inhibitors |
| Pain | Duloxetine Tricyclic antidepressants |
| Cognitive difficulties | Vortioxetine |
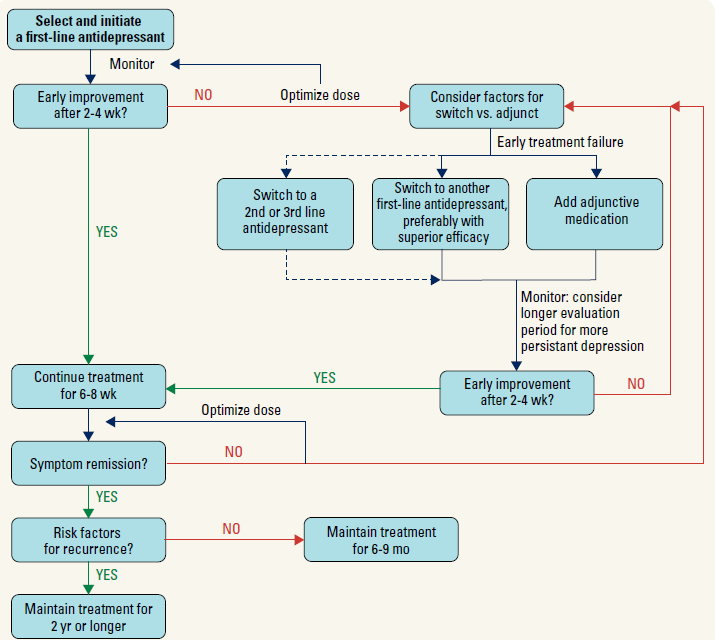
Treatment Approach for Depression
- optimization:
- increase dosage to maximum tolerated or highest therapeutic dosage
- augmentation:
- the addition of a medication that is not considered an antidepressant to an antidepressant regimen (i.e. thyroid hormone, lithium, atypical antipsychotics (aripiprazole, quetiapine, olanzapine, risperidone))
- combination:
- the addition of another antidepressant to an existing treatment regimen (i.e. the addition of bupropion or mirtazapine to an SSRI or SNRI)
- switch:
- change of the primary antidepressant (within or outside a class)
note: it is important to fully treat depression symptoms (i.e. to remission) to decrease relapse rates
Antidepressant adverse effects and their limitations on use
| Class | Major adverse effects | Ease of switching (half-life) | |||
| Weight gain | sedation/agitation | Sexual | Withdrawal syndrome | ||
| Selective serotonin reuptake inhibitors (SSRIs) | • | •• | ••• | ••† | •• |
| Serotonin noradrenaline reuptake inhibitors (SNRIs) | • | •• | ••• | ••• | •• |
| Serotonin modulator (vortioxetine) | • | • | •• | •• | ••• |
| Noradrenaline reuptake inhibitor (reboxetine) | • | • | •• | • | •• |
| Tricyclic antidepressants (TCAs) | ••• | ••• | ••• | ••• | ••• |
| Reversible inhibitor of monoamine oxidase A (moclobemide) | • | •• | • | • | ••• |
| Tetracyclic (mianserin) | •• | •• | • | •• | • |
| Noradrenergic and specific serotonergic (mirtazapine) | ••• | ••• | •• | •• | • |
| Monoamine oxidase inhibitors (MAOIs) | •• | ••• | •• | •• | ••• |
| Melatonergic (agomelatine) | • | • | • | • | • |
• Minimal limitation, •• Some limitation, ••• Marked limitation
Tricyclic Antidepressants
- Examples: Amitriptyline, Desipramine, Doxepin, Imipramine
- Pharmacokinetics:
- Metabolised in liver
- ½ life ~ 20hrs → long acting → takes 4-6 wks to judge if Tx is effective or not
- Adverse effects:
- Antimuscarinic/cholinergic effects:
- Dry mouth, blurred vision, constipation, urinary retention
- Delirium – in elderly or pts with Parkinson’s
- Sedation (H1 block)
- Confusion
- Postural hypotension
- Impotence
- tremor
- Acute toxicity – high risk (↑when combined with other CNS depressants)
- Cardiac arrhythmias – assoc with prolonged QT interval
- Seizures
- Mania
- Antimuscarinic/cholinergic effects:
- Contraindications:
- Pts with heart disease
- Pts on MAOIs
- Interactions with other drugs including:
- Alcohol, anaesthetics, antihypertensives & other drugs relying on hepatic metabolism for elimination → careful monitoring is v impt
- Clinical use is limited due to their side effects and the severity of acute overdoses, but they are more effective than newer drugs in treating severe depression
Selective Serotonin Reuptake Inhibitors (SSRIs)
- Most commonly prescribed antidepressants
- Examples: Fluoxetine, Fluvoxamine, Paroxetine, Sertraline, Citalopram, Escitalopram
- Pharmacokinetics:
- ½ life: 15-24 hrs → 2-4 wks before therapeutic effect develops
- Adverse effects:
- Nausea
- Insomnia
- Anorexia & wt loss/ weight gain
- CNS: restlessness, tremor, insomnia, headache, drowsiness, EPS
- GI: N/V, diarrhea, abdominal cramps,
- Sexual dysfunction: erectile dysfunction, anorgasmia,loss of libido
- CVS: increased HR, increased QTc, serotonin syndrome, SIADH, decreased platelet aggregation – inc risk of bleeding
- Serotonin Syndrome
- Occurs when used with MAOIs
- nausea, diarrhea, palpitations, chills, diaphoresis, restlessness, confusion, and lethargy but can progress to myoclonus, hyperthermia, rigor, and hypertonicity
- Can lead to death
- treatment: discontinue medication and administer emergency medical care as needed • important to distinguish from NMS
- Lack anticholinergic, adrenolytic & cardiac conduction effects like TCAs
- Contraindications:
- Should not be combined with MAO inhibitors → combination has lead to a few deaths
- Not used for children under 18 years of age
- ? ↑aggression
- ? ↑suicidal ideation at start of Tx
- Clinical uses:
- Depression
- Anxiety disorders
- Panic attacks
- Obsessive compulsive disorder
- Low risk of acute toxicity compared with TCAs, but less effective in treating severe depression
Serotonin & Noradrenaline Reuptake Inhibitors (SNaRIs)
- Examples: Venlafaxine, Duloxetine, Milnacipram
- Adverse effects:
- Similar to SSRIs
- Nausea in first 2 wks
- Effective in moderate to severe and refractory depression
- Safer in overdose than the TCAs
- May be faster onset of action than SSRIs and TCAs, but reason not clear
Noradrenaline Reuptake Inhibitor (NaRI)
- Examples: Reboxetine → not much clinical data validating use
- Adverse effects:
- Dizziness
- Insomnia
- Anticholinergic effects
- Headache.
- Lack or loss of appetite.
- Agitation, anxiety.
- Paraesthesia (pins and needles), inability to sit or stand still, altered taste sensation.
- Lack of visual focus.
- Increased heart rate, palpitations (heart pounding)
- Generally safer and fewer adverse effects when compared with TCAs
Noradrenaline and specific serotonin antidepressants (NaSSAs)
- mirtazapine, mianserin – chemically similar
- relatively safe in overdosage
- S/E
- fluid retention and swelling.
- CNS: sedation, dizziness, drowsiness, tiredness headache
- Endocrine: increase appetite, increase in cholesterol, increase in triglycerides, weight gain
- GI: constipation, ALT
Monoamine Oxidase Inhibitors (MAOIs) =Reversible, selective MAO inhibitors
- Examples: Moclobemide
- MOA: selectively and reversible inhibits MAO-A
- Adverse effects:
- Cheese reaction is not a problem
- Other adverse effects similar to the non-selective MAOIs
Bupropion
- active metabolite: hydroxybupropion
- MOA: ? ↑ dopaminergic and noradrenergic neuronal firing rates, but not serotonergic
- main disadvantage: risk of seizures
- improves abstinence rates for quitting smokers – ? why
Nefazodone, trazodone
- weak inhibition of NET (only by nefazodone) and SERT
- 5-HT2- receptor antagonist activity leads to antidepressant and anxiolytic effects
- 5-HT1B- receptor antagonist activity at presynaptic sites leads to increased 5-HT release
- relatively benign side effect profile except sedation
- effective in hospitalised depressed patients
Discontinuation Syndrome
- caused by the abrupt cessation of some antidepressants; most commonly with paroxetine, fluvoxamine, and venlafaxine (drugs with shortest half-lives)
- symptoms usually begin within 1-3 d and include: anxiety, insomnia, irritability, mood lability, N/V, dizziness, headache, dystonia, tremor, chills, fatigue, lethargy, and myalgia (“flu-like symptoms”)
::::FINISH:::
- Flu-like symptoms
- Insomnia Nausea
- Imbalance
- Sensory disturbances
- Hyperarousal (anxiety/agitation)
- treatment:
- symptoms may last between 1-3 wk, but can be relieved within 24 h by restarting antidepressant at the same dosage the patient was taking and initiating a slower taper over several weeks
- consider avoiding drugs with a short half-life
Non-pharmacological options
- Reassurance and listening
- Instill hope
- Consider Cork Analogy – Think of self as cork under water, No matter how much people or events push you under, Eventually you will pop up
- Reinforce Positive Behaviours
- Exercise (may increase energy and self esteem)
- Yoga
- Mindfulness Based Interventions
- Healthy Diet
- Attending Counseling
- Antidepressant Compliance
- Reassure that these are not habit forming
- Reassure that these are not forever
- Establish a therapeutic alliance
- Schedule pleasurable activities (esp. with people)
- Repair relationships with family and friends
- Consider keeping a journal
- Encourage good sleep hygiene
- regular bedtime and wake up time
- bed is for sleep and not for other activities (TV, social media).
- There are useful apps that provide basic psychoeducation and a sleep diary.
- Discourage Negative Behaviours
- Alcohol misuse = Encourage safe drinking. If there is heavy use and the patient is seeking treatment, refer to an addiction medicine service. If they are not seeking treatment, do a brief intervention.
- Substance misuse = Provide psychoeducation about the harmful effects of substances, advise abstinence, formal counselling or refer to addiction medicine services.
- Smoking = Encourage smoking cessation, and consider motivational interviewing and nicotine replacement therapy.
- Unhealthy diet = Psychoeducation about healthy diet and the harms associated with processed food. Encourage Mediterranean diet and increased intake of fruit and vegetables.
- Challenge negative thoughts
- Stress in relationships and work
- Educate family and patient
- Greatest risk of Suicide is in early treatment
- Cognitive Behavioral Therapy
- individual’s psychological problem has evolved from ‘faulty’ cognitions based on illogical beliefs with little or no rational basis.
- CBT aims to target these ‘illogical’ beliefs and replace them with more realistic beliefs that will help the patient overcome their illness.
- Efficacy: At least as effect as pharmacotherapy
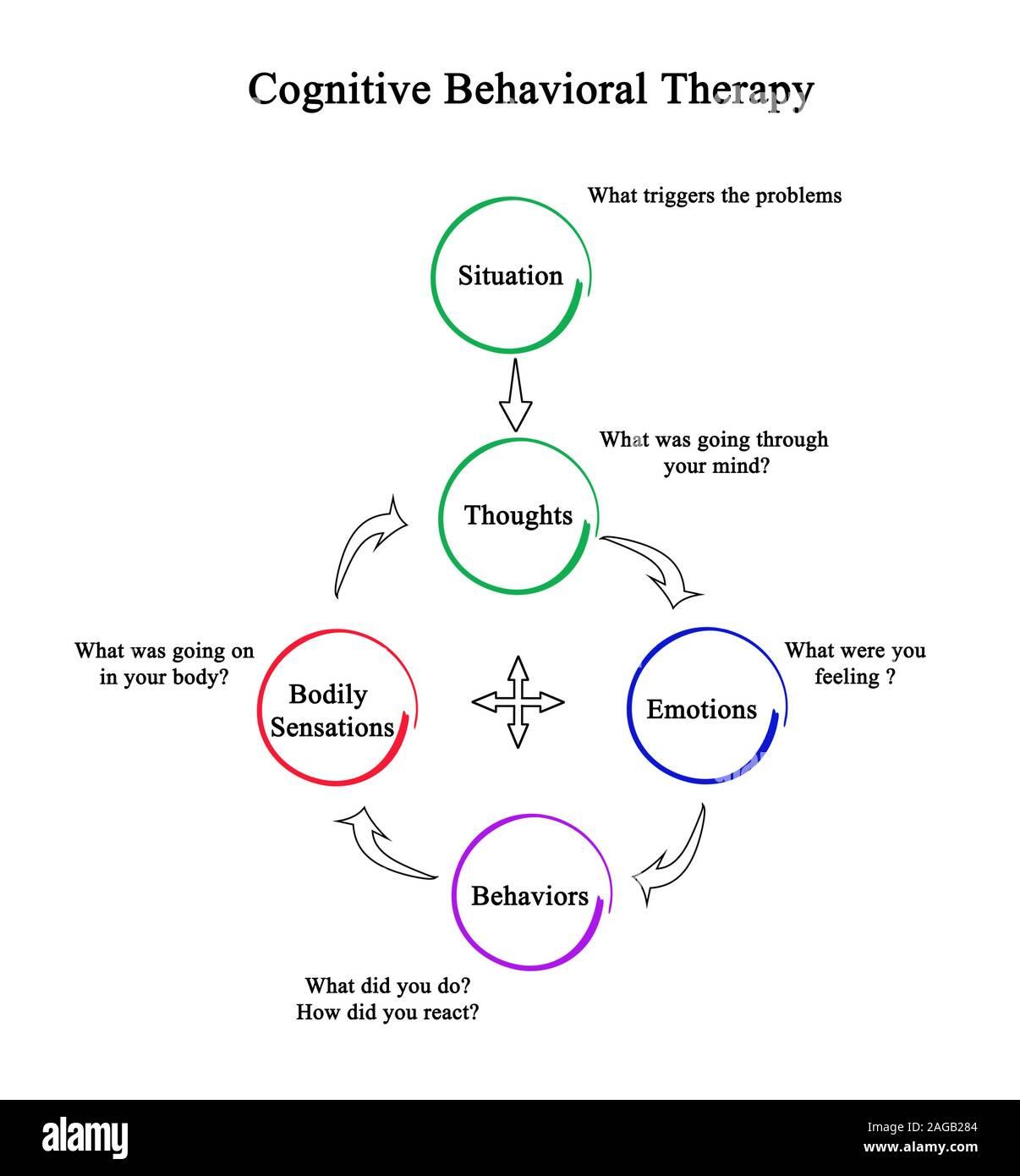
- Summary of Process
- Recognize that some Perceptions of reality are false
- All or Nothing thinking OR Black and White thinking: If I’m not the best I must be the worst; If I’m not a success I must be a failure etc
- Catastrophising: predicting personal future in a negative light
- Disqualifying positive events: positive events do not count in reasoning
- Emotional reasoning: I feel it therefore it must be true
- Magnification and minimisation: magnification of negative events, minimisation of positive events
- False Perceptions lead to negative thoughts
- Learn to identify negative thoughts as they occur
- Replace distorted thoughts with alternatives
- Reframe central beliefs about world and self-image
- Recognize that some Perceptions of reality are false
- Mindfulness-Based Therapy
- Mindfulness involves non-judgment, meaning that one pays attention to our thoughts and feelings with the attitude of an impartial witness – without believing them or taking them personally.
- Problem-solving therapy (PST)
- Short-term psychodynamic therapy (STPP)
- Keep a Thought Journal
- Set goals and activities – SMART
S -Specific- What will be accomplished? What actions will youtake?
M– Measurable- What data will measure the goal? (How much? How well?
A -Achievable – Is the goal doable? Do you have the necessary skill sand resources?
R – Relevant- How does the goal align with broader goals? Why isthe result important?
T -Time-Bound What is the time frame for accomplishing the goal?
- Adjuncts
- Website based cognitive-behavioral management
- Mood Gym
- http://moodgym.anu.edu.au
Management of specific subsets:
| Recommendations | |
| With anxious distress during the majority of days of a major depressive episode or persistent depressive disorder (dysthymia): Feeling keyed up or tense Feeling unusually restless Difficulty concentrating because of worry Fear that something awful may happen Feeling that the individual might lose control of himself or herself High levels of anxiety have been associated with higher suicide risk longer duration of illness and greater likelihood of treatment nonresponse | • Use an antidepressant with efficacy in generalized anxiety disorder (Level 4) • No differences in efficacy between SSRIs, SNRIs, and bupropion (Level 2) |
| With catatonic features hypoactive or decreased psychomotor activity (the most common type of catatonia) impaired: swallowing, dehydration, malnourishment from lack of eating, and risk of aspiration | • Benzodiazepines (Level 3) • No antidepressants have been studied |
| With melancholic features Loss of pleasure in all, or almost all, activities Lack of reactivity to usually pleasurable stimuli (does not feel much better, even temporarily, when something good happens) profound despondency, despair, empty mood Depression that is regularly worse in the morning Early-morning awakening (i.e. – at least 2 hours before usual awakening) Marked psychomotor agitation or retardation Significant anorexia or weight loss Excessive or inappropriate guilt | • No specific antidepressants have demonstrated superiority (Level 2) • TCAs and SNRIs have been studied |
| With atypical features Mood reactivity (i.e. – mood brightens in response to actual or potential positive events) Significant weight gain or increase in appetite Hypersomnia Leaden paralysis (i.e. – heavy, leaden feelings in arms or legs) interpersonal rejection sensitivity (not limited to episodes of mood disturbance) that results in significant social or occupational impairment | • No specific antidepressants have demonstrated superiority (Level 2) • Older studies found MAO inhibitors superior to TCAs |
| With psychotic features Delusions and/or hallucinations are present With mood-congruent psychotic features: all delusions and hallucinations is consistent with the typical depressive themes of personal inadequacy, guilt, disease, death, nihilism, or deserved punishment With mood-incongruent psychotic features: content of the delusions or hallucinations does not involve typical depressive themes of personal inadequacy, guilt, disease, death, nihilism, or deserved punishment, or the content is a mixture of mood-incongruent and mood-congruent themes | • Use antipsychotic and antidepressant cotreatment (Level 1) • Few studies involved atypical antipsychotics |
| With mixed features manic/hypomanic symptoms are present during the majority of days of a major depressive episode: Elevated, expansive mood Inflated self-esteem or grandiosity More talkative than usual or pressure to keep talking Flight of ideas or subjective experience that thoughts are racing. Increase in energy or goal-directed activity (either socially, at work or school, or sexually) Increased or excessive involvement in activities that have a high potential for painful consequences (e.g. – engaging in unrestrained buying sprees, sexual indiscretions, or foolish business investments) Decreased need for sleep (feeling rested despite sleeping less than usual; to be contrasted with insomnia) Mixed symptoms are observable by others and represent a change from the person’s usual behavior not attributable to the physiological effects of a substance (e.g. – a drug of abuse, a medication, other treatment) Mixed features associated with a major depressive episode have been found to be a significant risk factor for the development of bipolar I or bipolar II disorder. | • Lurasidone (Level 2) • Ziprasidone (Level 3) • No comparative studies and other somatic symptoms |
| With seasonal pattern egular temporal relationship with particular time of the year (e.g. – in the fall or winter). not include cases in which there is an obvious effect of seasonally related psychosocial stressors (e.g. – regularly being unemployed every winter). Full remissions also occur at a characteristic time of the year | • No specific antidepressants have demonstrated superiority (Level 2 and 3) •SSRIs, agomelatine, bupropion, and moclobemide have been studied |
| With cognitive dysfunction | • Vortioxetine (Level 1) • Bupropion (Level 2) • Duloxetine (Level 2) • SSRIs (Level 2) • Moclobemide (Level 3) |
| With sleep disturbances | • Agomelatine (Level 1) • Mirtazapine (Level 2) • Quetiapine (Level 2) • Trazodone (Level 2) |
| With somatic symptoms | • Duloxetine (pain) (Level 1) • Other SNRIs (pain) (Level 2) • Bupropion (fatigue) (Level 1) • SSRIs (fatigue) (Level 2) • Duloxetine (energy) (Level 2) |
Situational Depression
- (also known as Reactive Depression, Exogenous Depression, and Adjustment Disorder)
- depressive symptoms that occur when an individual is unable to adjust to or cope with a particular stress or a major life event.
- This was a previously historical diagnosis that has fallen out of clinical use. Its close counterpart is now called adjustment disorder, which reflects much of the same symptoms.