Obsessive-compulsive disorder (OCD)
- affects 2-3% of population at some time of lives
- a bimodal distribution
- ages 7-12 (males>females)
- age 21 (females>males).
- about 20% achieve remission in 40 years of follow up
- Poor prognostic factors include:
- early onset, poor insight, schizotypal features, and thought/action compulsions
- M=F
- Many don’t get help
- adapt and live with the Sx
Risk Factors
- etiology unknown but links to:
- neurological abnormalities: links to genetic:
- neurological dysfunction (brain injury, Sydenham’s or Huntington’s chorea)
- abnormal EEG
- abnormal evoked auditory potentials
- family history of OCD or Tourette’s disorder
- paediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS) in children following group A β-streptococcal infection; also linked to D8/17 antigenpositivity
- neurological abnormalities: links to genetic:
pts experience either
- obsessions or
- compulsions or
- both
Obsessions
- Recurrent and persistent thoughts, urges, or images
- intrusive and inappropriate
- cause marked anxiety or distress
- An attempt is made to ignore or suppress these or neutralise them with other thoughts or actions. (i.e. – by performing a compulsion)
- OCD patients will recognise them as a product of their own minds.
- Obsessions can be external or internal:
- External obsessions: contamination, objects, smells, asymmetry, mismatched items
- Internal obsessions: ego-dystonic thoughts (violent, sexual, etc.), always ask: “are these thoughts intrusive in nature?”
Common Obsessions
| Descriptions/Examples | |
| Contamination | Concerns about dirt, germs, body waste, illness |
| Symmetry | Needing things “just so”, even, or lined up a certain arbitrary way |
| Aggressive | Most commonly focused on inadvertent harm, such as being responsible for a fire or break-in; also includes horrific thoughts or images of deliberately harming others, such as stabbing a loved one or pushing a stranger in front of a car |
| Sexual | Disturbing sexual thoughts that are not consistent with an individual’s orientation or cultural norms, such as someone with a same-sex preference having unpleasant hetero-erotic thoughts, or unwanted inappropriate sexual thoughts about children |
| Religious | Examples include thoughts about selling one’s soul to the devil, deliberately thinking inappropriate thoughts about major religious figures, or committing mortal sins |
| Somatic | Exaggerated fears of contracting a serious illness such as hepatitis, or a brain tumour in the absence of any identifiable high risk |
Compulsions
- Repetitive behaviours (e.g. – hand washing, ordering, checking) or
- Mental acts (e.g. – praying, counting, repeating words silently)
- feel driven to perform in response to an obsession.
- my performing the compulsive behaviour, supposed to prevent or reduce distress but the relief is short-lived (thus they may be repeated many more times!)
- rituals eventually lose their power to relieve anxiety.
- Thus pts will develop more complex ones or take several hours to perform them
- OCD also associated with avoidance behaviour.
- The handicap in OCD is because the obsessions, compulsions and distress take up vast amounts of time.
Common Compulsions
| Descriptions/Examples | |
| Washing | Excessive hand-washing, showering, or cleaning activities |
| Checking | Repeatedly turning the stove on and off; re-reading all emails to ensure content is appropriate; driving around the block to ensure didn’t hit someone; asking for repeated reassurance |
| Ordering | Folding clothes “just so”, or arranging all cans in the cupboard so the labels are facing out |
| Counting | Performing actions a certain arbitrary number of times, such as tapping each foot 4 times when getting out of bed |
| Repeating | Repeatedly going up and down the stairs or flushing the toilet; typically done to “cancel” out a bad thought or until it feels “right” |
“Having OCD is MURDER” can be used to remember the criteria for obssessive-compulsive disorder
- M – Mind (patient aware symptoms arise in the mind)
- U – Unpleasant thoughts
- R – Resist (patient must want and try to resist the obsessive thoughts)
- D – Displeasure of feeling the obsession
- E – Ego-dystonic
- R – Repetitive thoughts
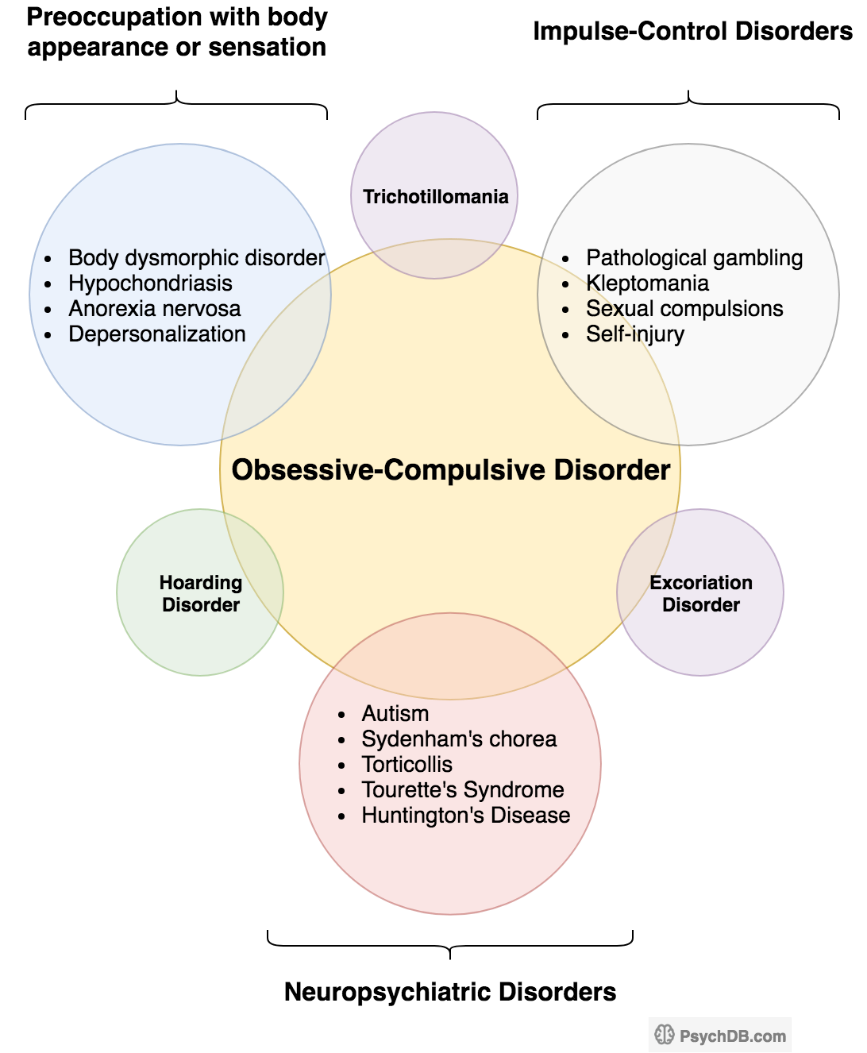
DDX to rule out
- excessive worries, as in generalized anxiety disorder
- preoccupation with appearance, as in body dysmorphic disorder
- difficulty discarding or parting with possessions, as in hoarding disorder
- hair pulling, as in trichotillomania
- skin picking, as in excoriation disorder
- stereotypies, as in stereotypic movement disorder
- ritualized eating behaviours, as in eating disorders
- preoccupation with substances or gambling, as in substance-related and addictive disorders
- preoccupation with having an illness, as in illness anxiety disorder
- sexual urges or fantasies, as in paraphilic disorders
- impulses, as in disruptive, impulse-control, and conduct disorders
- guilty ruminations, as in major depressive disorder
- thought insertion or delusional preoccupations, as in schizophrenia spectrum and other psychotic disorders
- or repetitive patterns of behaviours, as in autism spectrum disorder
Comorbidity
60-90% of individuals with OCD also have a comorbid mental disorder, including
- mood, anxiety
- somatoform disorders
- substance use disorders
- psychotic disorders
- bipolar disorders.
- In children, with OCD
- 5 to 7% incidence for Tourette’s
- 30% have a life-time history of tics.
- ADHD
- Many psychiatric and neuropsychiatric disorders also exist on the OCD spectrum
Management
- Exposure and Response/Ritual Prevention Therapy (ERP)
- Is a specialized form of CBT
- is the gold standard and first-line treatment for OCD
- patients are exposed to situations that trigger obsessions 🡪 and are taught strategies to prevent the compulsive response that would temporarily relieve their anxiety
- Patients gradually become desensitized to the feared stimulus, resulting in improved OCD symptoms.
- To do ERP successfully, patients must have significant buy-in into the therapy, as it can be a very distressing experience.
- Long-term maintenance of improvement has been shown in both children and adults.
Medications
- considered if CBT with ERP does not improve OCD symptoms
- 12-16 wk potential delay until response must be treated longer (at least 3 months)
- need doses near the maximum recommended doses
| 1st line | Monotherapy: escitalopram, fluoxetine, fluvoxamine, paroxetine, sertraline | Max doses: Clomipramine 150-250mg PO daily Fluoxetine 20-80mg PO daily Fluvoxamine 150-300mg PO daily Sertraline 100-200mg PO daily Paroxetine 20-80mg PO daily Escitalopram 10-50mg PO daily* Citalopram 20-80mg PO daily **QTc monitoring is recommended for doses of citalopram over 40mg and escitalopram over 20mg |
| 2nd line | Monotherapy: citalopram, clomipramine, mirtazapine, venlafaxine XR | |
| 3rd line | Monotherapy: IV citalopram, IV clomipramine, duloxetine, phenelzine, tramadol, tranylcypromine | |
| Adjunctive therapy | First-line: aripiprazole, risperidone Second-line: memantine, quetiapine, topiramate Third-line: celecoxib, citalopram, haloperidol, IV ketamine, mirtazapine, N-acetylcysteine, olanzapine, ondansetron, pindolol, pregabalin Not recommended: buspirone, clonazepam, lithium, morphine | |
| Not recommended | Clonazepam, clonidine, desipramine |
Related Disorders
Body Dysmorphic Disorder
- preoccupation with ≥1 perceived flaws in physical appearance not observed by others
- repetitive behaviours (e.g. mirror checking, excessive grooming, skin picking, or reassurance seeking) or mental acts (e.g. comparing self to others) related to appearance
- ± muscle dysmorphia
- causes clinically significant distress or functional impairment
- rule out eating disorder
- mean age of onset: 15
- symptoms tend to be chronic; high rate of suicidal ideation and attempts; comorbidity with MDD, social anxiety disorder, and OCD
Hoarding Disorder
- persistent difficulty discarding possessions regardless of actual value
- feels the need to save items, discarding creates distress
- results in possessions cluttering/compromising active living areas (may be uncluttered with 3rd party intervention, i.e. family member, cleaners, authorities)
- causes clinically significant distress or functional impairment
- rule out brain injury, cerebrovascular disease, Prader-Willi syndrome, OCD, MDD (low energy), psychotic disorder (delusions), neurocognitive disorder, ASD (restricted interests)
- tends to begin in teens and worsens over time, more common in older populations, large genetic component
Excoriation (Skin-Picking) Disorder
- recurrent skin picking resulting in lesions
- repeated attempts to stop or decrease skin picking
- causes clinically significant distress or functional impairment
- rule out scabies, substance use (e.g. cocaine), psychotic disorder (e.g. delusions, tactile hallucinations), body dysmorphic disorder, stereotypic movement disorder, non-suicidal self-injury
- treatment similar to trichotillomania (described above)
Trichotillomania (Hair-Pulling Disorder)
- recurrent pulling out own hair resulting in hair loss
- causes clinically significant distress or functional impairment
- different types of emotional states:
- Be triggered to pull hair by
- feelings of anxiety or boredom
- tension (either immediately before pulling out the hair or when attempting to resist the urge to pull)
- lead to gratification
- pleasure,
- sense of relief when the hair is pulled out.
- Be triggered to pull hair by
- Common
- scalp, eyebrows, and eyelids (less common sites are the facial, pubic, axillary, and peri-rectal regions
- The hair pulling occurs to the degree that significant hair loss occurs
- Epidemiology
- Prevalence is 1-2% in the general population.
- It affects significantly more females than males with a ratio of 10:1.
- Among children with trichotillomania, males and females are more equally represented.
- Prognosis
- Hair pulling may be seen in infants, but this behaviour typically resolves early in development.
- The onset of hair pulling seen in trichotillomania most commonly coincides with, or follows the onset of, puberty.
- The usual course of trichotillomania during this later onset is chronic, with waxing and waning of symptoms if the disorder is untreated (over periods of weeks, months, or sometimes years).
- Symptoms may worsen in females with hormonal changes (e.g. – menstruation, perimenopause).
- Some individuals may achieve full remission without relapse
- There may be irreversible damage to hair growth and hair quality for some individuals.
- If there is swallowing of pulled hair (trichophagia)
- this may lead to trichobezoars
- which lead to anemia, abdominal pain, hematemesis, nausea and vomiting, bowel obstruction, and/or perforation
- Comorbidity
- The majority of individuals also have one or more other body-focused repetitive behaviors, including skin picking, nail biting, and lip chewing.
- There is a high comorbidity with major depressive disorder, OCD, excoriation disorder, body dysmorphia, and tics.
- Differential Diagnosis
- Normative hair removal/manipulation
- Many individuals twist and play with their hair, but this behaviour does not usually qualify for a diagnosis of trichotillomania.
- Some individuals may bite rather than pull hair, which again, does not qualify for a diagnosis of trichotillomania.
- Obsessive-compulsive disorder
- Individuals with OCD and symmetry concerns may pull out hairs as part of their symmetry rituals, and individuals with body dysmorphic disorder may remove body hair that they perceive as ugly, asymmetrical, or abnormal.
- In these cases a diagnosis of trichotillomania is not given.
- Body-focused repetitive behaviour disorder
- Body-focused repetitive behavior disorder excludes individuals who meet diagnostic criteria for trichotillomania.
- Neurodevelopmental disorders
- In neurodevelopmental disorders, hair pulling may meet the definition of stereotypies (e.g. – in stereotypic movement disorder).
- Psychotic disorders
- Individuals with a psychotic disorder may remove hair in response to a delusion or hallucination. Trichotillomania is not diagnosed in such cases.
- medical condition
- alopecia areata
- androgenic alopecia
- telogen effluvium
- nonscarring alopecia (e.g. – chronic discoid lupus erythema tosus, lichen planopilaris, central centrifugal cicatricial alopecia, pseudopelade, folliculitis decalvans, dissecting folliculitis, acne keloidalis nuchae)
- Normative hair removal/manipulation
- Investigations
- Skin biopsy and dermoscopy
- Physical Exam
- Patterns of hair loss are highly variable in trichotillomania.
- Areas of complete alopecia, as well as areas of thinned hair density, are common.
- Eyebrows and eyelashes may be completely absent.
- If the scalp is involved, hair may most likely be missing in the crown or parietal regions.
- Treatment
- Pharmacotherapy
- TCA: Clomipramine (Anafranil), Olanzapine is useful
- SSRIs/SNRIs are generally ineffective for trichotillomania.
- Psychotherapy
- Habit reversal therapy (HRT) (a form of cognitive behavioural therapy) is the first-line treatment
- HRT’s premise is that the best way to shift a habit is to diagnose and retain the old cue and reward, and to try to change only the routine itself.
- HRT includes cognitive restructuring, awareness training, and behavioural analysis/identification of triggers, and developing competing responses.
- Habit reversal therapy (HRT) (a form of cognitive behavioural therapy) is the first-line treatment
- Pharmacotherapy