Post-traumatic stress disorder
- Diagnosis
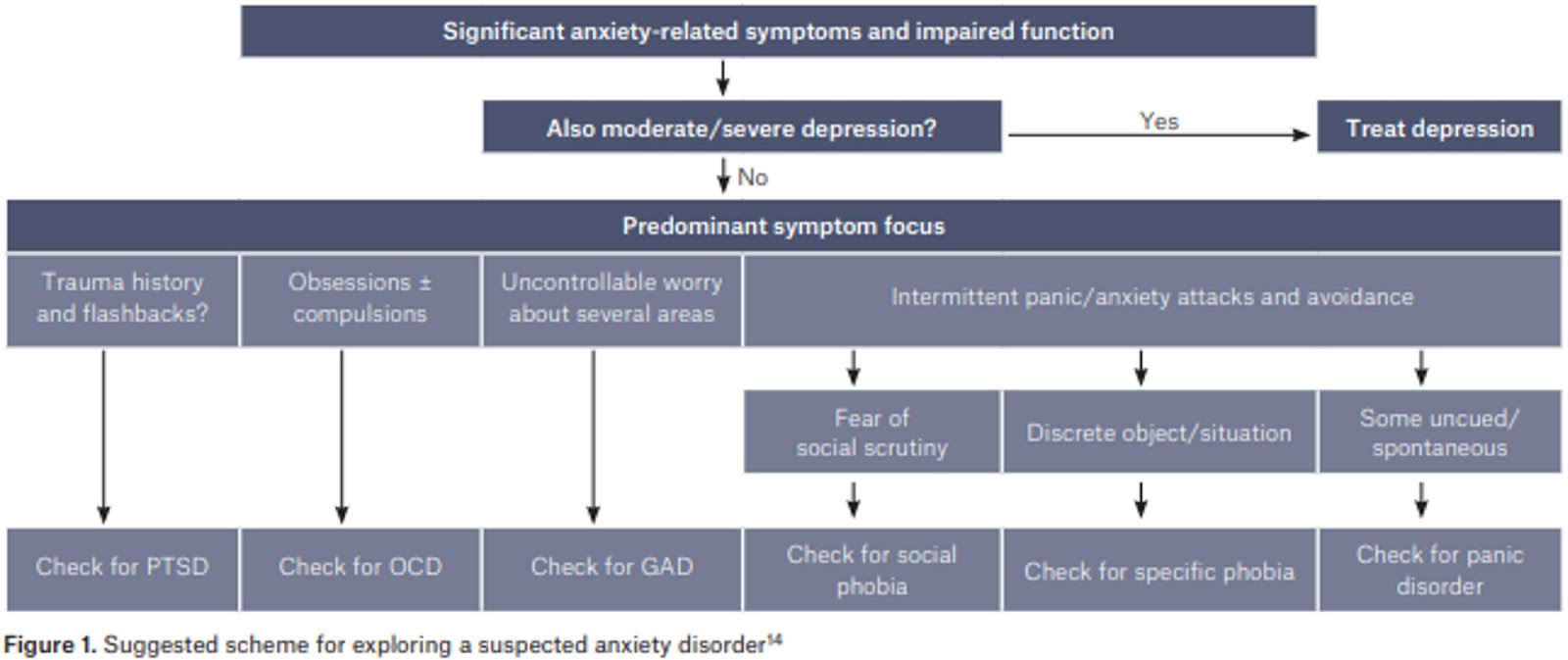
- Exposure to actual or threatened death, serious injury, or sexual violence in at least 1 of the following ways:
- Directly experiencing the traumatic event(s).
- Witnessing, in person, the event(s) as it occurred to others.
- Learning that the traumatic event(s) occurred to a close family member or close friend. – In cases of actual or threatened death of a family member or friend, the event(s) must have been violent or accidental.
- Experiencing repeated or extreme exposure to aversive details of the traumatic event(s) (e.g. – first responders collecting human remains or police officers repeatedly exposed to details of child abuse).
- Intrusion Symptoms
- Recurrent, involuntary, and intrusive distressing memories of the traumatic event
- children: older than 6 years, repetitive play may occur in which themes or aspects of the traumatic event(s) are expressed.
- Recurrent distressing dreams in which the content and/or affect of the dream are related to the traumatic event(s).
- children: there may be frightening dreams without recognizable content.
- Dissociative reactions (flashbacks) in which the individual feels or acts as if the traumatic event(s) were recurring.
- may occur on a continuum, with the most extreme expression being a complete loss of awareness of present surroundings
- children: trauma-specific reenactment may occur in play.
- intense or prolonged psychological distress at exposure to internal or external cues that symbolize or resemble an aspect of the traumatic event(s).
- Recurrent, involuntary, and intrusive distressing memories of the traumatic event
- Avoidance
- Avoidance of or efforts to avoid distressing memories, thoughts, or feelings about or closely associated with the traumatic event(s).
- Avoidance of or efforts to avoid external reminders (people, places, conversations, activities, objects, situations) that arouse distressing memories, thoughts, or feelings about or closely associated with the traumatic event(s).
- Negative Cognition and Mood
- Inability to remember an important aspect of the traumatic event
- dissociative amnesia
- Persistent and exaggerated negative beliefs/expectations about oneself, others, or the world
- e.g., “I am bad,” “No one can be trusted,” ‘The world is completely dangerous,” “My whole nervous system is permanently ruined
- Persistent, distorted cognitions about the cause or consequences
- individual to blame himself/herself or others.
- Persistent negative emotional state
- fear, horror, anger, guilt, or shame
- diminished interest or participation in significant activities.
- Feelings of detachment or estrangement from others.
- Persistent inability to experience positive emotions
- (e.g., inability to experience happiness, satisfaction, or loving feelings).
- Changes in Arousal
- Irritable behavior and angry outbursts = verbal or physical aggression toward people or objects.
- Reckless or self-destructive behavior
- Hypervigilance
- Exaggerated startle response
- Problems with concentration
- Sleep disturbance (e.g., difficulty falling or staying asleep or restless sleep).
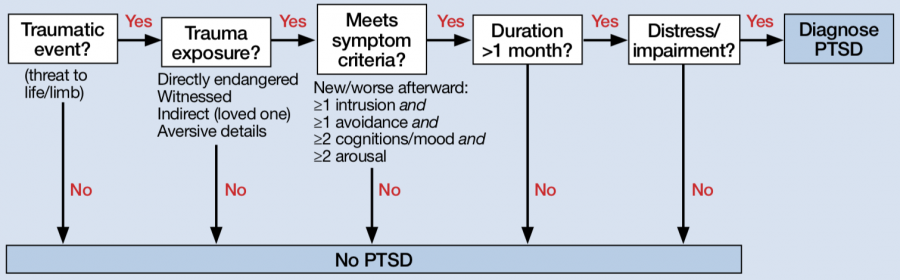
- Exposure to actual or threatened death, serious injury, or sexual violence in at least 1 of the following ways:
T – Traumatic event (experienced, witnessed, or was confronted, and the person experienced intense helplessness, fear, and horror)
R – Re-experiencing (intrusive thoughts, nightmares, flashbacks, or traumatic memories/images)
A – Avoidance (emotional numbing, detachment from others, flattening of affect, loss of interest, lack of motivation, and persistent avoidance of things associated with the traumatic experience)
U – Unable to function (symptoms cause negative mood, distress, or cause significant impairment in social, occupational, and interpersonal life)
M – 1 month of symptoms (at least)
A – Arousal increased (insomnia, poor concentration, irritable, angry, startle reflex, hypervigilance)
Prognosis
- PTSD can occur at any point in life, beginning after age 1.
- Symptoms usually begin within the first 3 months after trauma,
- although for some there may be a delay of months or years before the criteria for a full diagnosis is met.
- PTSD symptoms can be chronic, lasting years to decades after the initial trauma.
- However, individuals generally have substantially improved occupational functioning at work, relationships, and social interactions.
- long-term employment disability related to PTSD is also rare.
- Functioning
- functioning will improve significantly over the long term
- even if posttraumatic stress symptoms remain.
Risks
- increased risk for suicidal ideation and suicide attempts
- the risk is increased by 2 to 3-fold
Comorbidity
- 80% will have another mental disorder, including
- depressive disorders
- anxiety disorders
- substance use disorders
- borderline personality disorder.
- In children with PTSD
- oppositional defiant disorder
- separation anxiety disorder
Treatment
- Psychotherapy
- Cognitive processing therapy (CPT)
- trauma-focused CBT (TF-CBT)
- prolonged exposure (PE) therapy
- Eye movement desensitization and reprocessing therapy (EMDR)
Following treatment with psychotherapy, benefits can be maintained between 1 to 10 years.
In children, art therapy, play therapy, and family therapy (without the perpetrators of the trauma) can also be helpful.[
- Pharmacotherapy
- should start with either a selective serotonin reuptake inhibitor or a serotonin norepinephrine reuptake inhibitor.
- For individuals with PTSD-associated nightmares:
- Prazosin can reduce trauma nightmares and improve sleep quality. However, one recent randomized control trial actually found no difference between prazosin and placebo in military veterans with PTSD-associated nightmares.
- Naltrexone may also reduce flashbacks, and that fluphenazine may improve, we experiencing the symptoms.
| 1st line | Monotherapy: fluoxetine, paroxetine, sertraline†, venlafaxine XR |
| 2nd line | Monotherapy: fluvoxamine, mirtazapine, phenelzine |
| 3rd line | Monotherapy: amitriptyline, aripiprazole, bupropion SR, buspirone, carbamazepine, desipramine, duloxetine, escitalopram, imipramine, lamotrigine, memantine, moclobemide, quetiapine, reboxetine, risperidone, tianeptine, topiramate, trazodone |
| Adjunctive therapy* | Second-line: eszopiclone, olanzapine, risperidone Third-line: aripiprazole, clonidine, gabapentin, levetiracetam, pregabalin, quetiapine, reboxetine, tiagabine Not recommended: bupropion SR, guanfacine, topiramate, zolpidem |
| Not recommended | Alprazolam, citalopram, clonazepam, desipramine, divalproex, olanzapine (as monotherapy), tiagabine |
† = If there is a co-morbid substance use disorder, sertraline is recommended as the medication of choice, * = Adjunctive therapy is used in patients who have had an inadequate response to adequate antidepressant therapy, and can be considered for patients with treatment-resistant PTSD.
Doses of pharmacological agents in the treatment of PtsD
| Antidepressants | Doses (mg/day) |
| Paroxetine | 20–50 |
| sertraline | 50–200 |
| fluoxetine | 20–80 |
| Venlafaxine | 75–300 |
| Mirtazapine | 15–45 |
| amitriptyline | 50–300 |
| imipramine | 50–300 |
| Phenelzine | 15–75 |
| Anticonvulsants | Doses (mg/day) |
| topiramate | 25–500 |
| lamotrigine | 50–500 |
| Carbamazepine | 300–1000 |
| Antiadrenergic | Doses (mg/day) |
| Prazosin | 2–15 |
| Clonidine | 0.2–0.4 |
| Antipsychotics | Doses (mg/day) |
| risperidone | 0.5–6 |
| olanzapine | 5–20 |
| Quetiapine | 25–300 |