Ankylosing spondylitis
- Approximately 5% of chronic lower back pain
- progressive inflammation and stiffening of the spine
- male to female ratio is 3:1
- onset in AS is usually 20-30 years old and up to 95% of patients will present before 45 years old.
- Has a slow insidious onset
- delay between onset of symptoms and physician diagnosis of AS is 5–7 years on average
- Cause:
- The exact cause of AS is unknown, but there is suspected to be a strong genetic element with the involvement of the HLA-B27 gene.
- usually presents with early sacroiliac joint involvement leading to inflammatory back pain.
- This is followed by the involvement of the spine.
- In the spine, there is initial inflammation at the junction between the vertebrae and intervertebral discs. annulus fibrosis undergoes ossification and forms syndesmophytes
Clinical features
- Chronic lower back pain and morning stiffness are characteristic of AS.
- Clinical features usually start insidiously at a young age (< 45 years).
- Back pain characteristically
- occurs at night
- improves with exercise
- does not get better with rest.
- Morning stiffness
- Fatigue
- Alternating buttock pain
- Asymmetrical large joint peripheral arthritis, most often involving lower limb
- Physical exam:
- Increased occiput-to-wall distance
- Decreased chest expansion
- Loss of normal lumbar lordosis & increased thoracic kyphosis
- Painful sacro-iliac joint
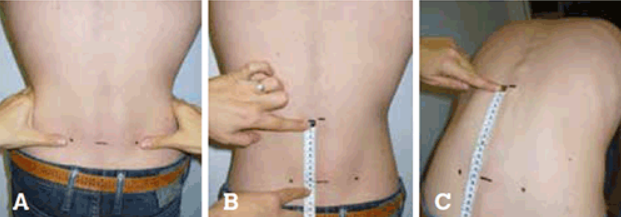
- Decreased Schroeber (decreased forward flexion of the lumbar spine)
Interpretation: Normal is > 5 cm increase in length. Less than 5 cm represents hypomobility
- Spinal deformity (seen in advanced disease)
- Extra-articular manifestations – seven ‘A’s’:
- Aortitis: aortic valve incompetence (up to 10%)
- Anterior uveitis (40%):
- inflammation of the middle layer of the eye (i.e. the uvea). Typically causes unilateral eye pain, redness, and photophobia.
- Seen in 25-35% of individuals with SpA
- Atrioventricular block
- Atlanto-axial instability: increases risk of cord compression
- apical pulmonary fibrosis (up to 15%)
- Amyloidosis: secondary to chronic inflammation
- IgA nephropathy
- Osteopenia and osteoporosis
Investigations
Imaging
- X-ray
- pelvis X-ray – X-ray changes at the sacroiliac joints must be present in order to establish a diagnosis of AS
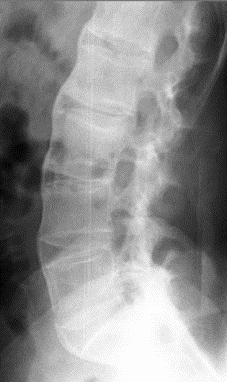
- Lumbar Xray – classic ‘bamboo spine’ is characteristic of advanced AS.
- The delay from symptom onset to X-ray changes, can be 10 years or more
- MRI
- Ultrasonography
- can be useful in detecting enthesitis, such as Achilles tendonitis
Laboratory tests
- ESR and CRP elevated in 50–70% of AS patients.
- HLA-B27
- occurs in 85–90% of patients.
- HLA-B27 is seen in 5–15% of the general population, with some variability associated with ethnic background,
- But 5% of HLA-B27 positive people develop AS.
- As such, HLA-B27 in the patient with clinical features of SpA can support the diagnosis but has no role as a general screening test for spinal pain
Diagnosis
- One of the most commonly used criteria to aid the diagnosis of AS is the 1984 Modified New York Criteria (validated in AS but now used in all SpA with axial involvement):
- Clinical criteria
- Age of onset <45y, Low back pain ≥ 3 months, improved by exercise and not relieved by rest
- Limitation of the lumbar spine in sagittal and frontal planes
- Limitation of chest expansion (relative to normal values corrected for age and sex)
- Radiological criterion
- Bilateral grade 2-4 sacroiliitis OR unilateral grade 3-4 sacroiliitis
- Diagnosis
- Definite ankylosing spondylitis: radiological criterion is present plus at least 1 clinical criterion
- Probable ankylosing spondylitis: if EITHER radiological criterion OR 3 clinical criteria are present alone
Treatment:
- As with any chronic condition, patient education and support is vital in the management of AS.
- The basic objectives of treatment are:
- prevention of spinal fusion in a poor position
- relief of pain and stiffness
- maintenance of optimum spinal mobility
- The basic methods of management are:
- advice on good back care and posture
- general education and counselling
- exercise programs to improve the range of movement and maintain mobility
- referral to physiotherapist
- drug therapy
- NSAIDs are first-line therapy for symptomatic AS patients.= regular NSAID use in AS slows radiographic progression more than on-demand use
- TNF inhibitor therapy
- as strikingly improved the quality of life for the more than two thirds of AS patients with an inadequate response to NSAIDs
- Other DMARDs (methotrexate and sulfasalazine)
- have little effect in spinal disease, but can be useful for an associated peripheral arthritis