OSTEOARTHRITIS
Epidemiology
- Most common arthropathy
- Over 50% of people over the age of 65 years have radiological evidence of disease
- approximately 10% of men and 18% of women have symptomatic OA
- Joint pain and reduced mobility cause considerable impact on quality of life
- with no current cure for this condition, general practitioners are left with a range of management options aimed at
- optimizing quality of life
- self-management
- preventing acute episodes
- delaying complications
- preventing progression of the condition
Pathogenesis
- Genetic predisposition
- Abnormal physical forces leading to altered joint function and damage. The primary event is deterioration of articular cartilage due to local biomechanical factors & release of proteolytic & collagenolytic enzymes (develops when cartilage catoblism > synthesis and loss of proteoglycans and water exposes underlying bone)
- Abnormal bone metabolism further damages joint – subchondral sclerosis, osteonecrosis & cyst formation, bone grows beyond joint margin (osteophytes (spurs))
- Synovitis is secondary to cartilage damage
Classification:
- Primary (idiopathic) – most common, aetiology unknown
- Secondary
- Post-traumatic/mechanical
- Post-inflammatory
- Heritable skeletal disorders (e.g. scoliosis)
- Endocrine disorders (e.g. acromegaly, hyperparathyroidism, hypothyroidism)
- Metabolic disorders (e.g. gout, haemochromatosis, Wilson’s disease)
- Neuropathic (Charcot joints – atypical joint trauma due to loss of proprioceptive senses (diabetes, syphilis))
- Avascular necrosis (fracture, steroids, alcohol, gout, sickle cell)
- Other (e.g. congenital malformation)
Assessment
- Effect on person’s function, quality of life, occupation, mood, relationships and leisure activities
- History of presenting symptoms and pain assessment
- Red flags: Signs and symptoms of infection, history of cancer, unexpected weight loss and fractures
- Medication use, doses, frequency, effectiveness and side effects
- Quality of sleep and fatigue
- Psychological factor
- Health beliefs, concerns, expectations and knowledge
- Modifiable risk factors (eg obesity, physical activity)
- Comorbidities
Clinical Features
- Age > 40
- Signs and symptoms localised to affected joints (not a systemic disease)
- Pain is often insidious and gradually progresses over years
- Flare ups and remissions may occur
| Symptoms | Signs |
| Joint pain with motion, relieved with rest Short duration of stiffness after immobility(less than 30 mins morning stiffness) Joint instability/buckling Loss of function Joint locking due to “joint mouse” (loose piece of bone in joint) | Joint line tenderness, stress painBony enlargements at affected joints Malalignment/deformity (angulation) Limited ROM Periarticular muscle atrophy Crepitus on passive ROM |
Joint involvement


- Can be any joint, especially knee, hip, hand, spine (less common are shoulder, elbow, wrist, ankle)
- Hand
- DIP (Heberden’s nodes = osteophytes → enlargement of joints)
- PIP (Bouchard’s nodes)
- CMC (usually thumb)
- MCP is often spared
- Hip
- Dull or sharp pain in trochanter, groin, anterior thigh or knee
- Internal rotation and abduction are lost first
- Knee
- Narrowing of one compartment of the knee is the rule (medial > lateral) – standing x-rays must be done
- Foot – most common in 1st MTP
- Lumbar spine
- Very common (esp. L4-5, L5-S1)
- Degeneration of fibrocartilaginous IV discs possibly with disc herniation or listhesis (slippage) and facet joint degeneration
- Reactive bone growth can complication neurological impingement
- Sciatic
- Neurologic claudication (spinal stenosis)
- Cervical spine
- Common, especially lower areas → neck pain
Laboratory results:
- Lab results are normal – normal FBC, ESR (negative RF, ANA)
- Radiology (4 classic findings)
- Narrowing of joint space
- Geode formation (intraosseous cysts)
- Subchondral sclerosis (“seagull sign” – whiter than normal area on each side of the bone)
- Osteophytes


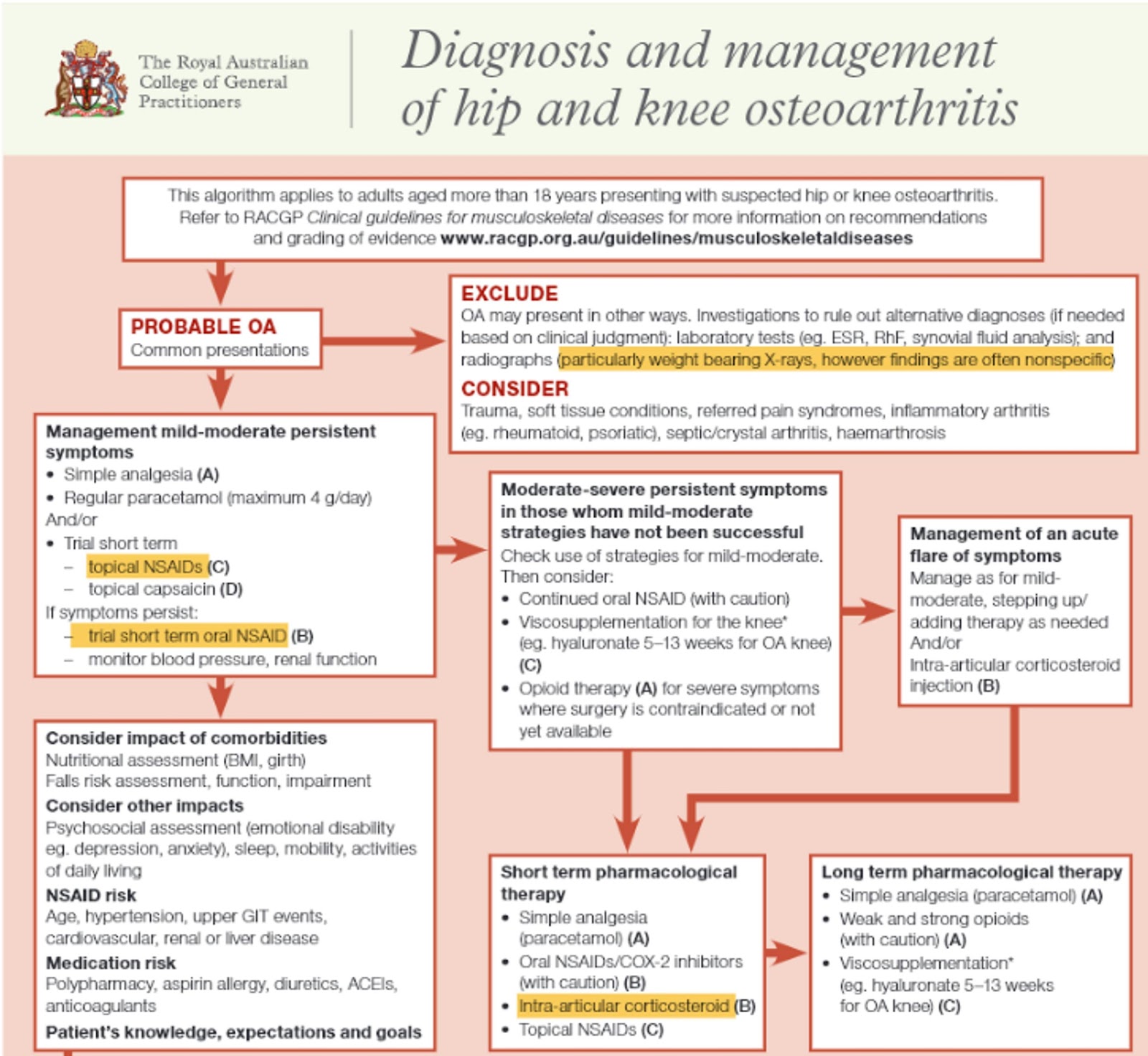
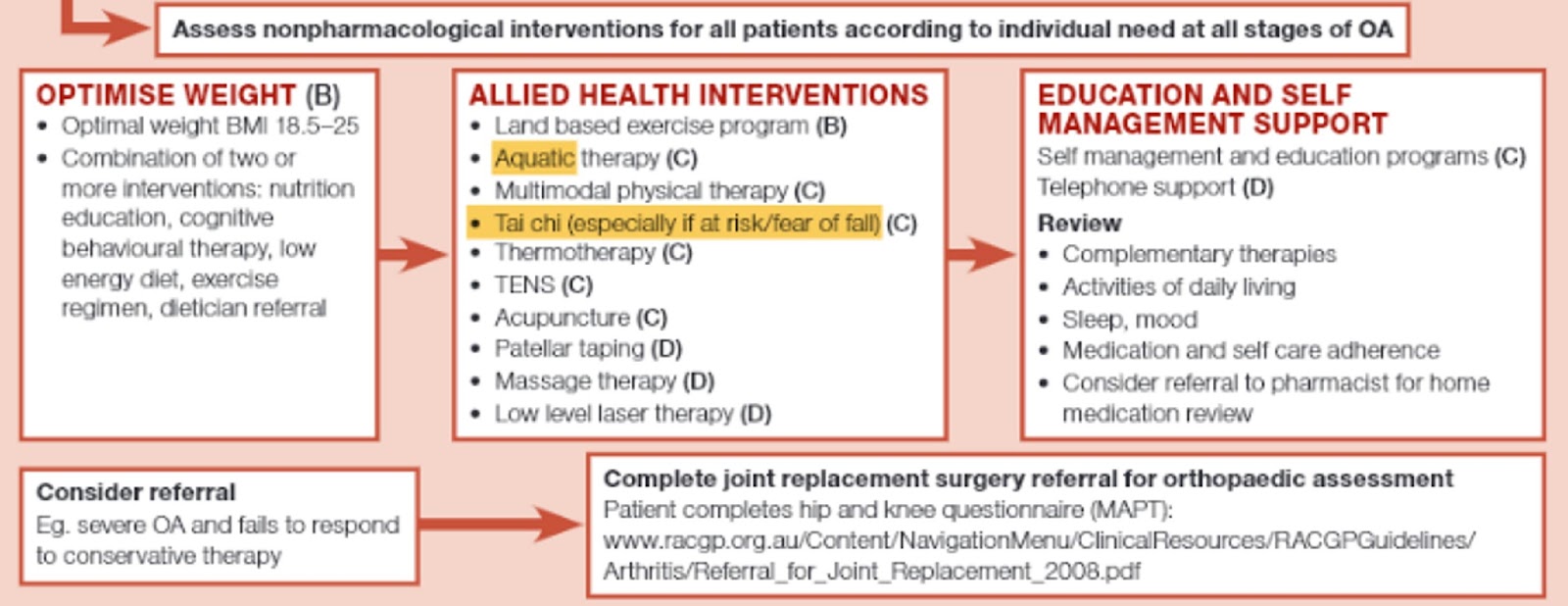
Management:
- No treatment alters the natural history
- Long term Mx
- Education
- Land-base exercise
- Weight loss – aim for loss ≥5% body weight if overweight or obese
- Optional adjunctive management – Trial for short term and cease if ineffective
- Aquatic-based exercise
- Thermal therapy (ie heat pad)
- Massage, manipulation and mobilisation
- Assistive walking devices
- Cognitive behavioural therapy (CBT) for pain coping or psychological symptoms
- Transcutaneous electrical nerve stimulation (TENS)
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- Advanced pharmacological attempts – Trial for short term if symptom still persistent
- Intra-articular corticosteroid if a flare of symptoms or rapid pain relief is required
- Duloxetine (off-label use
AIM
- optimizing quality of life
- nutritional education
- low energy diet
- Exercise
- land-based exercise
- Targeted muscle strengthening and general aerobic exercises
- water-based exercises suggested for those with functional and mobility limitations
- exercise provides benefit even if weight loss is not achieved
- has a role in both symptom management and as a preventive strategy
- self-management
- Patients with OA should be provided with information about their condition and advised about appropriate support groups.
- social, environmental and psychological interventions may be appropriate depending on the patient’s individual needs
- refer to Arthritis Australia
- managing and preventing acute episodes
- pharmacological
- Regular paracetamol (maximum 4 g/day) (1st line)
- NSAIDS (2nd line)
- COX-2 inhibitors (Celecoxib) (high risk group for GI bleed: >65, GI bleed/PUD, CV disease)
- Intra-articular corticosteroids
- (short-term effect)
- Topical capsaicin can be used as an alternative or as an adjunct to standard drug treatment.
- Reviews of RCTs found that topical capsaicin is superior to placebo for knee osteoarthritis and reduces pain by 50%
- Nonpharmacological
- physiotherapy
- OT (aids, splints, cane)
- pharmacological
- delaying complications/preventing progression of the condition
- weight reduction reduces disability in patients with OA
- Regular follow up of patients with established OA
- ongoing patient education
- review of multidisciplinary care
- medication review
- behavioural modification
total hip arthroplasty and total knee arthroplasty
