Osteomyelitis
- Classification
- Long or vertebral
- Long bone usually in children
- haematogenous spread to the well vascualrised metaphyseal bone adjacent to the growth plate
- Vertebral osteomyelitis
- Aka discitis, spondylodiscitis
- Usually older adults
- Haematogenous seeding vertebral endplate
- Secondary spinal and paraspinal collections
- Spinal epidural abscess can exist without osteomyelititis
- Long bone usually in children
- Long or vertebral
- Time course – acute or chronic
- Acute – new infection, absence necrosis and sequestra, usually < 14 days
- Chronic – relapsed or longstanding, often has a sinus, compromised soft tissue envelope, low grade inflammation, sequestra or involcurum (new bone formation adjacent to sequestra)
- Causes – adults
- Staph aureus most common
- Other organisms
- Coag negative staph, strep, enterococci, Enterobacteriaceae, pseudomonas
- More commonly atypicals if vertebral infection
- Atypical organisms more common in patients with other risk factors
- Post-op infection
- Recent UTI
- hepatobiliary or GI infection
- Healthcare associated infection
- IVDU
- Causes – children
- Almost always staph aureus
- Rarely HiB if not fully vaccinated
- Investigations
- Aim for microbiological diagnosis
- Blood cultures – 50% will have bacteraemia – at least 2 sets
- specimen – bone/pus – open or radiological biopsy
- Start empirical treatment whilst awaiting results
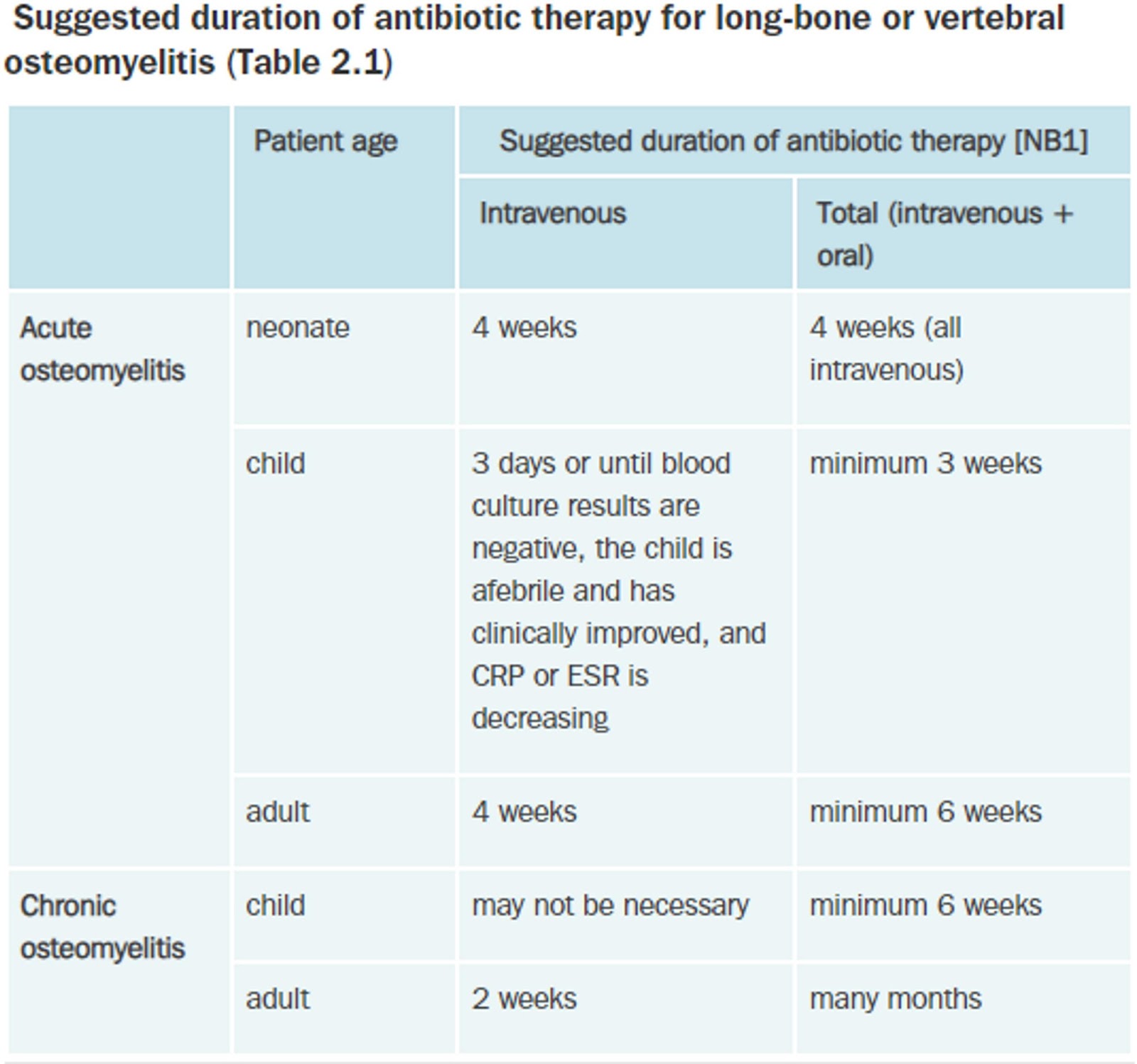
- Treatment
- Apart from non-complicated vertebral – can await results
- Adults – long bone
- Treat suspected staph – fluclox 2g 6hrly
- Suspect MRSA – vancomycin
- Adult – vertebral
- If well/no complications/normal neuro – await culture – fluclox
- If abscess or compromised – fluclox + vanc + ceftriaxone
- Adult – contigous with leg or foot ulcers
- Treat as diabetic foot infection
- Augmentin if well
- Piptaz if sepsis
- Children
- Flucloxacillin 50mg/kg 6hrly
Further follow up
- BMD before initiating corticosteroid treatment
- adequate supplementation of calcium (1200 mg/day) and vitamin D3 (cholecalciferol, 800 IU/day)
- If BMD T-score is –1.5 or less consider an oral bisphosphonate such as alendronate (70 mg/week) or risedronate sodium (35 mg/week).
- Referral to a rheumatologist should be considered if atypical features are present.