Systemic Lupus Erythematosus
Disorder characterised by inflammation in several organ systems and the production of auto-antibodies that participate in immunologically-mediated tissue injury.
- Peripheral polyarthritis with symmetric involvement of small and large joints WITHOUT joint erosion
Epidemiology:
- F;M = 10:1
- Age on onset is in reproductive years: 13-40 (more common in Blacks and Asians)
- Bimodal mortality pattern:
- Early (within 2 years): Active SLE, active nephritis, infection secondary to steroid use
- Late (>10 years): Inactive SLE, inactive nephritis, atherosclerosis possibly 2° to long-term steroid use
Proposed aetiology
- Altered immunity – too many autoAbs causing damage by cytotoxic effects of Ag-Ab complexes and/or altered regulating mechanisms (e.g. decreased T suppressor cells)
- 10% have family history
- Role of oestrogen
- Infection – virus
- Drug induced SLEs – minocycline anticonvulsants, phenytoin, methyldopa, antihypertensives (hydralazine), antiarrhythmics (procainamide), OCP can exacerbate = . Disease often regresses when the offending drug is discontinued.
Triggers:
- Sun Exposure: Ultraviolet (UV) light from the sun can trigger SLE flares, particularly skin rashes and other symptoms. This is why sun protection is crucial for people with SLE.
- Stress: Emotional or physical stress is often reported as a trigger for SLE flares. Stress management techniques may help in reducing the frequency or severity of flares.
- Fatigue: Overexertion and lack of rest can contribute to the onset of a flare. Maintaining a balanced lifestyle with adequate rest is important.
- Infections: Viral or bacterial infections can stimulate the immune system and potentially trigger a flare. Good hygiene and avoiding sick contacts when possible are preventive strategies.
- Certain Medications: Some medications can induce or exacerbate SLE symptoms. These might include certain antibiotics, blood pressure medications, and even some anti-seizure medications. It’s important for people with SLE to inform all healthcare providers about their condition to avoid such medications.
- Hormonal Changes: Hormonal fluctuations, such as those during menstruation, pregnancy, or menopause, can sometimes trigger SLE flares.
- Diet: While there’s no specific diet that causes SLE flares, some individuals may find that certain foods exacerbate their symptoms. Keeping a food diary can help identify any potential food triggers.
- Environmental Factors: Other environmental factors like exposure to certain chemicals or pollutants might play a role in triggering flares, though this is less well-understood.
- Smoking: Smoking can exacerbate SLE symptoms and is associated with more severe disease.
- Cold or Extreme Weather: Some people with SLE find that extreme weather conditions, such as cold or heat, can trigger symptoms.
Presentations

SLE can present is various ways depending on the system(s) that it affects. Common clinical manifestations include:
- Constitutional: fevers, malaise, lethargy, weight loss. Exclude other more serious pathologies.
- Cutaneous:
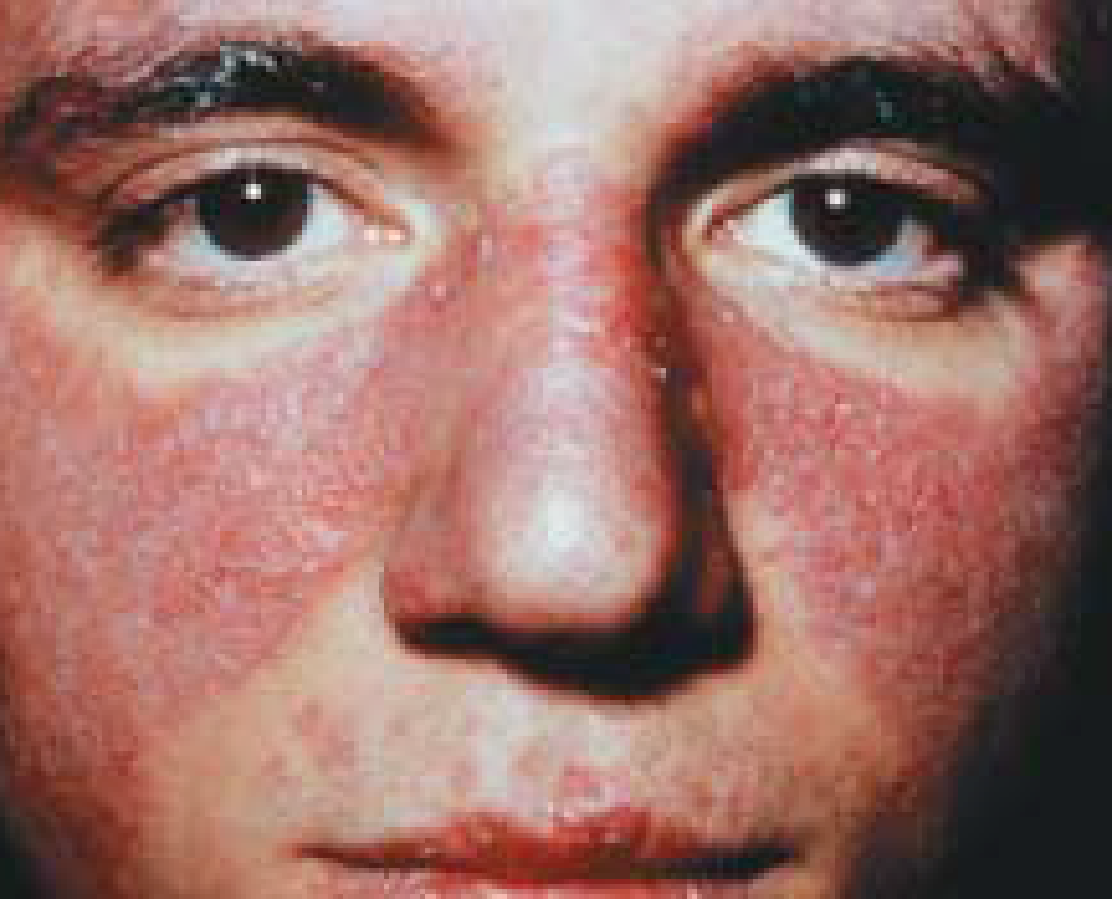
- Acute malar (‘butterfly’) rash
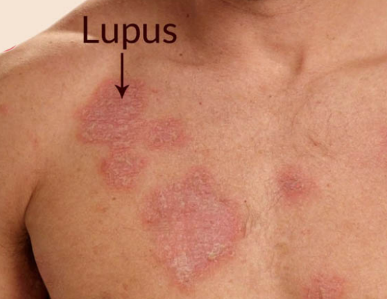
- discoid rash
- subacute cutaneous lupus rash (photosensitive)
- Alopecia
- Raynaulds
- oral ulcers
- vasculitis
- nail-fold infarcts
- MSK:
- 95% of SLE sufferers have intermittent arthritis: usually symmetrical polyarthritis affecting the PIPJ, MCPJ, wrists, and knees.
- Myalgia is common; but myositis is uncommon.
- Renal involvement (lupus nephritis) is a serious disorder:
- Occurs 30-50% of cases.
- May be silent: DO URINE! Urinalysis may show proteinuria and red cell casts. Biopsy may occasionally be necessary.
- Haematological:
- Anaemia (chronic disease / haemolysis / CKD)
- Leukopenia / lymphopenia / thrombocytopenia
- Serosal and cardiopulmonary manifestations: pleural effusions, ascites, pericarditis, pulmonary fibrosis, Libman-Sacks endocarditis.
Diagnostic criteria (4 of the 11 must present serially or simultaneously):
Clinical criteria:
- Malar rash: Classic “butterfly rash” – no scarring involved since BM intact
- Discoid rash: May cause scarring
- Photosensitivity
- Oral/nasal ulcers – usually painless
- Arthritis – non-erosive, symmetric, involving 2 or more small/large peripheral joints
- Serositis – pleurisy, pericarditis, peritonitis
- Neurologic disorder – headache, seizures, psychosis, neuropathy or cytoid body (cotton wool exudates on fundoscopy due to infarction of nerve cell layer of the retina)
Laboratory criteria
- Renal disorder – proteinuria, cellular casts (Hb, rbc, granular, tubular or mixed) – >0.5g/day or 3+
- Haematologic disorder – haemolytic anaemia, leukopenia, lymphopenia, thrombocytopenia
- Immunologic disorder – positive LE cell preparation, anti-dsDNA Ab, anti-Sm Ab,
- Antinuclear antibody – most sensitive test
Note: Often present with malaise and constitutional symptoms as well
Mnemonic: ‘SOAPBRAIN MD’:
- (S)erositis
- (O)ral ulcers
- (A)rthriti
- (P)hotosensitivity
- (B)lood derangement
- (R)enal disorder
- (A)NA +ve
- (I)mmunologic
- (N)eurological
- (M)alar Rash
- (D)iscoid Rash
Other associated features:
- Skin manifestations – urticaria, livedo reticularis, bullae, panniculitis, alopecia
- Vasculitic lesions – periungual telangiectasia, Raynaud’s
- Eye manifestations – conjunctivitis, episcleritis, keratoconjunctivitis
- Neuropsychiatric – personality disorders, depression, psychoes
NB: Drug induced SLE often presents atypically with systemic features and serositis. Usually associated with anti-histone antibodies.
Tests
- ANA highly sensitive
- 98% of patients with SLE with have raised ANA
- Anti-dsDNA is highly specific for ANA.
- Anti-Sm highly specific for SLE but poor sensitivity.
- C3 and C4 may be reduced
- FBC (may show reduced cell counts)
- UEC and urinalysis: to detect renal involvement
- Testing for antiphospholipid syndrome (can be associated with SLE, but also can be primary):
- anti-cardiolipin
- lupus anticoagulant
- b2-glycoprotein 1.\\
- Anti-histone
- is specific for drug-induced lupus but is not sensitive
ANA testing are reported in two components:
- the quantity of ANA in the serum (intensity)
- most commonly reported as a titre, reflecting the final step in a series of two-fold dilutions at which the ANA remains positive
- 1:1280 for a strongly positive ANA
- 1:160 for a weaker, borderline positive ANA
- most commonly reported as a titre, reflecting the final step in a series of two-fold dilutions at which the ANA remains positive
and, when the ANA is positive:
- the pattern of antibody binding to the nucleus (staining pattern)
| ANA pattern | Associated rheumatic disease |
| Homogeneous | Systemic lupus erythematosus Mixed connective tissue disease Drug induced lupus Juvenile idiopathic arthritis |
| Speckled | Systemic lupus erythematosus Sjögren’s syndrome Polymyositis/dermatomyositis Systemic sclerosis/scleroderma |
| Nucleolar | Diffuse systemic sclerosis/scleroderma Polymyositis |
| Centromere | Limited systemic sclerosis/scleroderma |
| Peripheral (rim) | Systemic lupus erythematosus Systemic sclerosis/scleroderma |
- ANA test is highly sensitive for certain rheumatic diseases such as
- SLE
- systemic sclerosis/scleroderma
- But negative result doesn’t exclude a wide range of other conditions including
- rheumatoid arthritis
- spondyloarthropathies
- idiopathic inflammatory myopathies
- vasculitides.
- Many patients with autoimmune disease will not have a positive ANA
- Changes in the ANA level
- are not associated with autoimmune disease activity
- repeat testing should not be performed unless there has been a significant change in the clinical picture.
- Positive ANA is seen in a range of conditions where it is not diagnostically helpful
- Low-intensity titre ANA
- are present in up to 40% of healthy individuals.
- moderate titre ANA
- 5% of the healthy population have a moderate titre ANA that is considered positive
- chronic infection
- viral hepatitis
- malignancy
- Low-intensity titre ANA
- some autoimmune conditions (such as multiple sclerosis or thyroid disease)
- the presence or absence of ANA does not play a significant role in diagnosis or prognosis.
- If ANA positive ,need follow-up testing for ENA antibodies
| Sensitivity of ANA for rheumatic diseases | |
| Disease | Sensitivity (%) |
| Systemic lupus erythematosus | 93 |
| Systemic sclerosis/scleroderma | 85 |
| Polymyositis/dermatomyositis | 61 |
| Juvenile idiopathic arthritis | 57 |
| Juvenile idiopathic arthritis with uveitis | 80 |
| Sjögren’s syndrome | 48–73 |
| Rheumatoid arthritis | 41 |
Management principles:
- Treat early using the mildest form possible then slowly withdraw therapy
- If higher doses of steroids are necessary for long term control, use steroid sparing agents as well, then taper steroids if possible
- Use bisphosphonates, Ca, vitamin D if steroids are used
Treatment:
- Symptomatic treatment tailored to organ system involved and severity
- Patient education – sunscreen, avoid UV light and oestrogens
- NSAIDS – arthritis, pleurisy, pericarditis
Topical therapy
- Intermittent courses of potent topical corticosteroids are important in the treatment of CLE. They should be applied accurately to the skin lesions.
- The calcineurin inhibitors tacrolimus ointment and pimecrolimus cream can also be used.
Systemic therapy
Treatment of SLE depends on which are the predominant organs involved in the disease. Typically, any of the following drugs may be used alone or in combination.
- Systemic corticosteroids, such as prednisone or prednisolone. These are the mainstay of treatment in a seriously ill patient with acute LE. prevent end organ damage secondary to inflammation
- Hydroxychloroquine if SLE w/o serious internal organ involvemen
- Hydroxychloroquine and other antimalarials—response rates are about 80% in CLE.
- Methotrexate
- Immunosuppressives
- azathioprine
- mycophenolate
- cyclophosphamide
- Intravenous immunoglobulin
- Aspirin is recommended for antiphospholipid syndrome.
- Targeted biologic therapies under evaluation for SLE include
- anifrolumab
- belimumab
- rituximab
CLE is also sometimes treated with:
- Retinoids (isotretinoin and acitretin)
- Dapsone.
Considerations in Pregnancy
- Conception should be planned around the time that the disease is stable.
- Presence of anti-phospholipid syndrome increases miscarriage rate (indeed, it is in the definition of APLS) – may need regular aspirin and LMWH during pregnancy.
- Presence of anti-Ro and anti-La (which can cross placenta) increases risk of neonatal lupus – defined by transient rash, cytopenia, hepatitis, and congenital heart block.
Monitoring Disease Activity
- Anti-dsDNA can be used to monitor disease activity, particularly renal involvement.
- Rising anti-dsDNA with decreasing C3 suggest flareup.
- There is usually no need to measure ANA again in an individual who has been confirmed to have SLE.
Non-Pharmacological management
Preventative measures
The following measures are essential to reduce the chance of flares and organ damage.
- Careful protection from sun exposure using clothing, accessories and SPF 50+ broad-spectrum sunscreens. Sunscreens alone are not adequate.
- Smoking cessation
- Rest when needed.
- Lifestyle Modifications:
- Sun Protection: UV light can trigger SLE flare-ups. Using sunscreens with high SPF, wearing protective clothing, and avoiding excessive sun exposure are crucial.
- Smoking Cessation: Smoking can worsen SLE symptoms and increase the risk of cardiovascular diseases. Quitting smoking is strongly recommended.
- Balanced Diet: A healthy diet can help manage SLE. Omega-3 fatty acids, found in fish and flaxseeds, may be beneficial. It’s also important to limit foods high in saturated fats, salt, and sugar
- Stress Management:
- Techniques like mindfulness, meditation, and yoga can help reduce stress, which is known to exacerbate SLE symptoms.
- Exercise:
- Regular, moderate exercise can improve overall health, reduce stress, and help in managing joint and muscle pain. Activities like walking, swimming, or cycling are often recommended.
- Allied Health – offer physical and functional support, focusing on pain reduction, joint protection, muscle strengthening, and overall improvement in the quality of life
- Physiotherapy:
- Aims to improve muscle strength and encourage mobility in affected joints.
- Techniques used include heat, cold, and electrotherapy to reduce pain and inflammation.
- Exercise therapy is crucial in maintaining or increasing joint mobility and overall physical health (Akil & Amos, 1995).
- Physiotherapy significantly augments medical therapy by improving the management of RA, reducing daily living handicaps for patients (Kavuncu & Evcik, 2004).
- Occupational Therapy:
- Focuses on educating patients to protect their joints and improve function through exercise and the use of aids and appliances.
- Provides splints when necessary to support affected joints.
- Helps patients adapt to lifestyle changes and maintain or improve psychosocial health.
- Aims at improving performance in daily living tasks and facilitating successful adjustments in lifestyle
- Physiotherapy: