Vasculitis: Large Vessel
- Giant cell arteritis
- Polymyalgia rheumatica
- Takayasu arteritis
- Behcet syndrome
Giant Cell Arteritis
Introduction
Also called temporal arteritis or cranial arteritis
Clinical syndromes: polymyalgia rheumatica and temporal arteritis 20% association between temporal arteritis and PR
Symptoms:
- Constitutional Symptoms:
- Weight loss
- fever, fatigue
- anorexia
- malaise are common.
- Headache:
- New-onset or worsening headaches are typical, though not present in all cases.
- Jaw Claudication:
- Pain while chewing or talking.
- Temporal Artery Abnormality:
- Enlargement, tenderness, nodular swelling of temporal artery.
- Visual Symptoms:
- Vision loss is usually sudden and painless
- due to anterior ischemic optic neuropathy caused by vasculitis involving the ophthalmic artery or the posterior ciliary arteries
- can be initially unilateral or bilateral, and there is a high risk of bilateral vision loss if unilateral vision loss is not urgently treated with high-dose corticosteroids
- other: double vision, and amaurosis fugax.
- Vision loss is usually sudden and painless
- Polymyalgia Rheumatica (PMR):
- Joint and muscle pain, often involving shoulder and hip girdles.
- Neurological Symptoms:
- Transient ischemia
- strokes
- mononeuropathies.
- Respiratory Symptoms:
- Cough, sore throat, hoarseness.
- Extracranial Symptoms:
- Involvement of other arteries, leading to claudication, bruits, aneurysms.
- Polymyalgia Rheumatica (PMR)
- Both PMR and GCA share similar pathogenesis. PMR is characterized by synovitis and periarthritis involving the shoulder and hip girdles, leading to pain, stiffness, and loss of range of motion of the bilateral shoulder and hip girdles.
- PMR can occur before, with, or after GCA. Further, 40 to 60% of GCA patients have PMR, and 15 to 20% of PMR patients have GCA
| ACR diagnostic criteria for GCA |
| Age >50 years |
| New onset of localised headache |
| Temporal artery tenderness or decreased temporal artery pulse |
| ESR ≥50 mm/hr |
| Positive temporal artery biopsy |
Pathophysiology
Type of collagen disease causing inflammation of extracranial vessels
Diagnosis
- Biopsy and histological exam of superficial temporal artery.
- Elevated ESR and CRP
- anemia
- thrombocytosis.
- MRI high Sn and Sp.
- Consider this Dx with new headache.
Treatment
Corticosteroids – Mainstay of treatment, aiming to prevent vision loss. High initial doses tapered over time.
- Prednisolone 40–60mg (not <0.75 mg/kg) continued for 4 weeks (until resolution of symptoms and laboratory abnormalities)
- Reduction by 10 mg every 2 weeks to 20 mg
- Reduction by 2.5 mg every 2–4 weeks to 10 mg
- Reduction by 1 mg every 1–2 months provided there is no relapse
- reduce according to clinical state using ESR/CRP
- start treatment immediately to prevent permanent blindness
- Symptoms of GCA often improve within days to weeks of starting treatment, but the duration can vary from person to person
- TA may take 1-2 years to resolve.
DxT: fatigue + headache + jaw claudication = temporal arteritis
Complications:
- Irreversible vision loss – Untreated GCA can cause irreversible vision loss due to damage to the optic nerve
- aortic aneurysms – : Inflammation of the aorta can lead to the weakening of the vessel wall and the development of aneurysms or dissections.
- cerebrovascular events, including strokes – Overall, about 1 to 3% of patients with temporal arteritis die from a stroke or an MI
- complications from Steroids: The biggest problem with the treatment of temporal arteritis today is the morbidity associated with corticosteroids
Polymyalgia Rheumatica
Inflammatory condition of unknown aetiology
Characterised by aching and morning stiffness in the cervical region and shoulder and pelvic girdles
Epidemiology:
- Incidence 50/100 000 per year in those over 50
- Age of onset >50, F:M = 2:1
- Giant cell (temporal arteritis) and PR are closely related
HLA-DRB1*04 associated with temporal arteritis but not directly with PR
Clinical Features
- Hallmark: hip girdle pain with pronounced stiffness
- Stiffness and an aching pain mainly affecting the
- shoulder girdle, neck and pelvic girdle
- Morning stiffness can last at least 30 minutes
- Shoulder pain
- is the most common presenting symptom (70-95% of patients
- Hip and neck involvement is about 50-70%.
- Pain worse with movement Bilateral
- Radiates distally from the shoulder and pelvic girdle Can be severe enough to interfere with sleep
- Limitation of movement mainly due to pain rather than weakness
- Signs may be absent later in the day
- Constitutional symptoms prominent (weight loss, malaise, fever)
- Morning stiffness of proximal muscles and joints (neck, hip, shoulder, thighs)
- Physical examination reveal tender muscles but no weakness or atrophy
- Lab – anaemia, ↑ ESR/CRP, normal CK
DxT: malaise + painful shoulder girldle + morning stiffness (>50yo) = polymyalgia rheumatica
Diagnosis
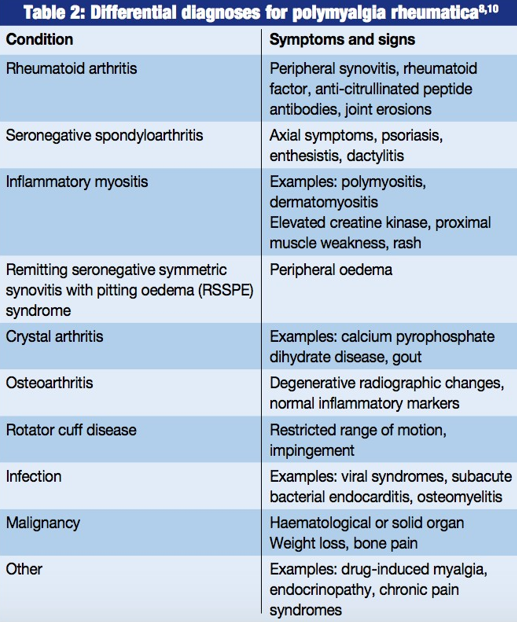
- Must rule out infection, RA, SLE, PAN, malignancy & giant cell arteritis
| Classification criteria for PMR | |
| BSR and BHPR guidelines (2009) | New EULAR/ACR classification (2012) |
| Age >50 years, duration >2 weeks | Age ≥50 years with new bilateral shoulder pain |
| Bilateral shoulder or pelvic girdle aching, or both | New hip involvement (pain, tenderness, limited movement) |
| Morning stiffness for >45 min | Morning stiffness for >45 min |
| Evidence of an acute-phase response | Elevated C-reactive protein and/or ESR |
| Normal inflammatory markers if there is a classical clinical picture and response to steroids | In the absence of peripheral synovitis or of positive RA serology |
| Ultrasound findings of bilateral shoulder abnormalities (subacromial bursitis, bicipital tenosynovitis, glenohumeral effusion) or abnormalities in one shoulder and hip (hip effusion, trochanteric bursitis) | |
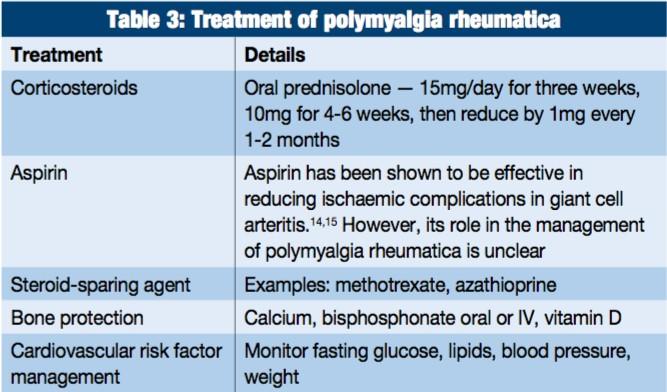
Treatment
clinical response criteria :
- improvement in morning stiffness
- ability to raise the arms above shoulder height consistent with the patient’s baseline mobility before onset of polymyalgic symptoms
- improvement in the patient and doctor’s global assessment (preferably performed on a visual analogue scale)
- reduction in the C-reactive protein or ESR (or both)
- Corticosteroids treatment may take 1-2 years
- usually self-limiting
- In patients with relapses, a rapid improvement of symptoms is generally observed following the resumption or an increase in the dose of prednisolone.
Up to 50% of patients experience at least one relapse during the course of their disease
| BSR/BHPR prednisolone-tapering regimen for GCA and PMR | |
| GCA | PMR |
| Prednisolone 40–60mg (not <0.75 mg/kg) continued for 4 weeks (until resolution of symptoms and laboratory abnormalities) | Prednisolone 15 mg for 3 weeks |
| Reduction by 10 mg every 2 weeks to 20 mg | 12.5 mg for 3 weeks |
| Reduction by 2.5 mg every 2–4 weeks to 10 mg | 10 mg for 4–6 weeks |
| Reduction by 1 mg every 1–2 months provided there is no relapse | Reduction by 1 mg every 4–8 weeks or alternate day reductions (eg. 10/7.5 mg alternate days) |
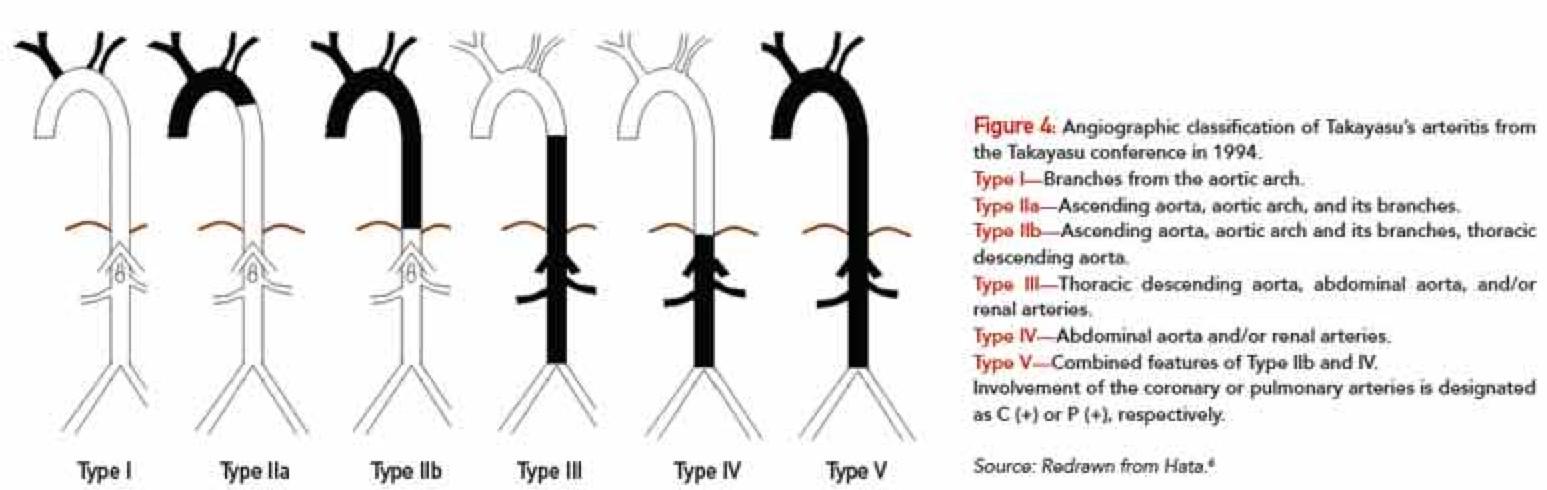
Takayasu arteritis
Introduction
- aka “pulseless disease” or “aortic arch syndrome” Involves the aortic arch and other major arteries Affects young Japanese female adults typically
Features
- Absence of peripheral pulses Hypertension
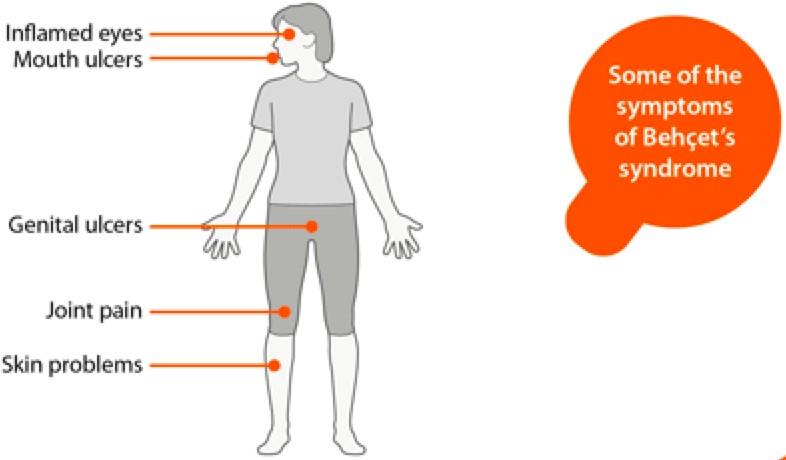
Behcet syndrome
Introduction
- Systemic (multiorgan) vasculitis of unknown aetiology Affects veins and arteries of all sizes
Main Feature
- Painful oral ulceration
- Hallmark is the “pathergy” reaction
- simple trauma such as a pinprick can cause a papule or pustule to form within a few hours at this site
Clinical Features
- M:F = 2:1
- Recurrent oral and/or genital ulceration
- Arthritis (usually knees)
- Ocular symptoms – pain, reduced vision, floaters (ocular inflammation)
- No specific diagnostic test
- Treatment: high dose steroids
- Associated complications: repeated uveitis and retinitis 🡪 blindness, colitis, venous thrombosis, meningoencephalitis
Wegener Granulomatosis
- Multisystem disease with necrosis, granuloma formation, and vasculitis.
- Affects upper/lower respiratory tract and kidneys (glomerulonephritis).
- Upper airway symptoms: sinusitis, nasal disease, otitis media, hearing loss, subglottic stenosis, ear pain, oral lesions.
- Lower respiratory tract symptoms: infiltrates, nodules, haemoptysis, pleuritis.
- Renal involvement can lead to chronic renal failure.
- Other symptoms: orbital mass, necrotising scleritis.
- Diagnosis: positive cytoplasmic staining (cANCA) with anti-proteinase-3 (PR-3) specificity and tissue biopsy.
Treatment:
- Severe Disease: immunosuppressants (corticosteroids, cyclophosphamide).
- Limited Disease: corticosteroids and methotrexate; frequent monitoring for severe disease progression.
- Exclusive upper airway involvement: treatment with trimethoprim+sulfamethoxazole.
Churg-Strauss Vasculitis
- Often preceded by atopy or asthma.
- Symptoms: fever, anorexia, abdominal pain, weight loss, asthma, respiratory infiltrates, eosinophilic infiltration.
- Common features: mononeuritis multiplex, skin manifestations (purpura, skin infarcts, nodules), myocardial/cardiac issues, renal involvement.
- Diagnosis indicators: blood eosinophilia (>1 × 10^9/L), positive perinuclear staining (pANCA), elevated creatinine.
Treatment:
- Oral corticosteroids for induction of remission.
- Indications for cyclophosphamide: proteinuria (>1 g/day), elevated serum creatinine (>0.14 mmol/L), cardiomyopathy, gastrointestinal involvement, CNS involvement.
- Treatment follows principles outlined in “Remission with cyclophosphamide”.