Vitamin D deficiency – Rickets
- Vitamin D is essential for bone and muscle health. Low vitamin D and low calcium and/or phosphate can cause nutritional rickets
- Sunlight is the most important source of vitamin D at all ages
- Vitamin D deficiency is common in risk groups and should be self-managed wherever possible – through education, behaviour change and supplementation as required
- In Australia, nutritional rickets is generally only seen in infants and children with dark skin
Background
- Sunlight (UVB) is the most important source of vitamin D (>90%) through skin synthesis of D3. This varies with
- Skin colour: people with dark skin require greater UVB exposure compared to people with light skin
- Skin exposure: covering clothing may result in low vitamin D levels
- Season/UVB availability: during winter there may not be enough UVB to maintain adequate vitamin D levels in southerly latitudes. Sunscreens do not result in low vitamin D with normal use
- Only small amounts of vitamin D are available from diet:
- the main natural food source is fish
- breastmilk, despite its other benefits, contains almost no vitamin D
- infant formula is fortified with vitamin D
- In the absence of sun exposure, recommended intakes of vitamin D are:
- 0–12 months old: 400 units daily
- 1–18 years old: 400–600 units daily
- 25-OH-D is used to measure vitamin D status
- The recommended 25-OH-D level is ≥50 nmol/L at all ages and during pregnancy
| Definitions of vitamin D status | |
| Severe deficiency | <12.5 nmol/L |
| Moderate deficiency | 12.5–29 nmol/L |
| Mild deficiency | 30–49 nmol/L |
| Sufficient | ≥50 nmol/L |
| Elevated | ≥250 nmol/L Toxicity is defined as serum 25-OH-D >250 nmol/L with hypercalcaemia and suppression of parathyroid hormone (PTH) |
Assessment
- Risk factors
- Lack of skin exposure to sun (time inside, covering clothes)
- Dark skin
- Medical conditions affecting Vitamin D metabolism (obesity, liver/renal failure, severe malabsorption, medications)
- Infants: exclusive breastfeeding AND any of: the above risk factors, maternal deficiency or prematurity
- History
- Time outdoors and covering clothing
- Dietary history (calcium intake, breastfeeding/formula in infants)
- Previous vitamin D levels and treatment
- a wide range of formulations are available
- Family understanding
- Non-specific bony/muscular pain, fatigue with exercise
- Poor growth, motor delay and irritability (infants)
- Symptoms of low calcium: muscle cramps, tetany, stridor, seizures (rare beyond 6–12 months of age)
- Examination
- Growth parameters, exclusion of other musculoskeletal pathology
- Delayed dentition (no teeth by 9 months, no molars by 14 months)

- Rickets:
- occurs in growing bones, so it mostly occurs in infants and young children, but it can also occur in teenagers 🡪 softer bones weaker bones – bend and become an abnormal shape
- long bone deformity (eg genu varum/valgus – if weight bearing)
- widening of wrists/ankles
- delayed anterior fontanelle closure (normally closed by 2 years)
- frontal bossing
- rosary (widening of ribs at costochondral junction)
- increased risk of fracture

Management
Flowchart – Investigation and treatment of low vitamin D
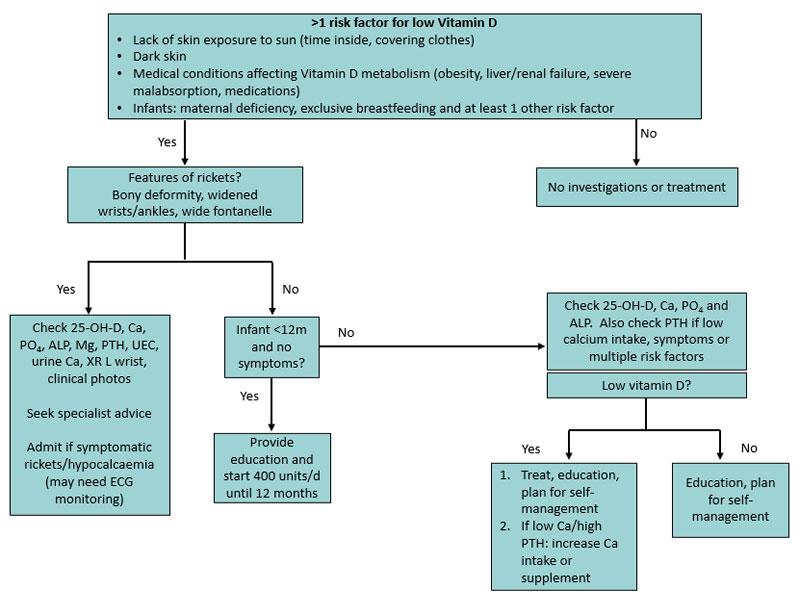
- Breast fed infants <12 months with other risk factors can usually start supplements (400 units daily) without investigations, provided they do not have symptoms/signs
- Consider admission: symptomatic hypocalcaemia (including tetany, stridor, seizures) or severe rickets
- Specialist review: infants with symptoms/signs, clinical rickets, abnormal serum calcium, or vitamin D deficiency not responding to high dose supplements
Investigations
- Breastfed babies can usually be started on supplements without testing
- Screen children/adolescents with one or more risk factors for low vitamin D (25-OH-D, Ca, PO4, and ALP)
- Also check PTH if low calcium intake, symptoms, or multiple risk factors
- Infants and children with rickets need additional investigations:
- 25-OH-D, Ca, PO4, ALP, Mg, PTH, UEC, urine Ca, PO4, creatinine; X-ray L wrist, clinical photos
- X-ray changes of rickets – osteopenia, metaphyseal widening/splaying/fraying
Treatment
- Children with low vitamin D should be treated (see table below) to restore their levels to the normal range (≥50 nmol/L)
- There is limited evidence to support high dose treatment in infants <3 months
- Ensure adequate calcium intake (see calcium intake table below) . Cheese, yoghurt and fortified soy dairy are useful sources of calcium in children who dislike cow milk. Consider supplements if poor intake
- Education on sun protection and exposure (see sun exposure table below). Children/young people with dark skin can tolerate intermittent sun exposure without sunscreen, although hats/sunglasses are still recommended
- Children with nutritional rickets should be managed under specialist guidance. The minimum recommended dose of vitamin D is 2000 units daily for minimum of 3 months, together with oral calcium 500 mg daily (either via diet or supplements). Phosphate supplements may also be needed
Treatment of low vitamin D
| Age | Level (deficiency) | Treatment Oral doses D3/colecalciferol 1 microgram = 40 units | Maintenance/prevention in children with ongoing risk factors |
| Preterm | Mild 30–49 nmol/L | 200 units/kg/day, maximum 400 units/day | 200 units/kg/day, maximum 400 units/day |
| Moderate or severe <30 nmol/L | 800 units/day, review after 1 month | ||
| <3 months (term) | Mild 30–49 nmol/L | 400 units/day for 3 months | 400 units daily |
| Moderate or severe <30 nmol/L | 1,000 units/day daily for 3 months | ||
| 3–12 months | Mild 30–49 nmol/L | 400 units/day for 3 months | 400 units daily |
| Moderate or severe <30 nmol/L | 1,000 units/day for 3 months OR 50,000 units stat and review after 1 month (consider repeating dose) | ||
| 1–18 years | Mild deficiency 30–49 nmol/L | 1,000-2,000 units/day for 3 months OR 150,000 units stat | 400–600 units daily, OR 3000–4000 units once weekly, OR 150,000 units at start of Autumn |
| Moderate or severe <30 nmol/L | 1,000–2,000 units daily for 6 months OR 3,000–4,000 units daily for 3 months OR 150,000 units stat and repeat at 6 weeks |
Calcium intake
| Age | Adequate intake (AI) | Estimated average requirement (EAR) | Recommended dietary intake (RDI) |
| 0–6 months | 200 mg | ||
| 7–12 months | 270 mg | ||
| 1–3 years | 360 mg | 500 mg | |
| 4–8 years | 520 mg | 700 mg | |
| 9–11 years | 800 mg | 1000 mg | |
| 12–18 years | 1050 mg | 1300 mg |
Ongoing monitoring and self-management
- Breastfed infants at risk of low vitamin D should be given 400 units vitamin D daily for at least the first 12 months
- Supplementation is usually not required in fully formula fed infants
- Follow up bloods (25-OH-D, Ca, PO4, ALP, and PTH if previously elevated)
- Not usually required in mild deficiency
- Check at 1 month in infants, at 3 months if older
- Children with risk factors for low vitamin D require ongoing monitoring and a plan to maintain vitamin D and calcium status with behavioural change and supplementation as required
- Provide education and a plan for self-management: consider 400–600 units daily OR 3000–4000 units once weekly over the cooler months (May–August) to avoid need for blood testing and the need for high dose therapy