Hepatitis A
- RNA virus
- virus shed in large quantities in the stool of infected persons.
- It can survive for weeks in water, marine sediment, shellfish or soil, and can persist on the hands for several hours and much longer in food kept at room temperature.
- It is also resistant to heat and freezin
- Transmission
- Fecal- oral transmission
- occasional transmission through sexual contact and blood transfusions
- Incubation 15-50 days
- Infectious from 2 weeks before prodrome to one week after jaundice or two weeks after prodrome
- Fecal shedding may continue for months although not necessarily infectious
- Usually a subclinical or self limited 3-6 weeks
Risks
- poor hygiene
- overcrowding
- Contaminated food or water Fomites
- Sexual activity / MSM
- Overseas travellers Childcares/preschool Residential facilities MSM
- IVDU ATSI
Epidemiology
- Risk for Travelers: Major hazard for individuals from low endemicity areas traveling to medium and high endemicity regions.
- Common in Travelers: Second most common vaccine-preventable infection in travelers after influenza.
- Effect of Vaccination: Widespread vaccination use has led to a significant decrease in cases, with a 75% reduction in imported hepatitis A cases reported in Swiss data from 1988–2004.
Incidence Rates
- Decline Over Time: Incidence among travelers to high-risk regions reduced to 3–11 per 100,000 person-months, a significant drop from rates before vaccine availability.
- Source Countries: High incidence from travel to Fiji, Philippines, India, Indonesia, and Pakistan.
Risk Variability by Traveler Type
- Accommodation and Lifestyle Factors:
- Non-immune travelers in high-standard hotels in endemic regions remain vulnerable.
- Budget travelers, backpackers, and trekkers face up to six times greater risk.
- Prolonged Stays: Higher infection rates observed among those staying long-term in endemic areas, such as US missionaries in Africa.
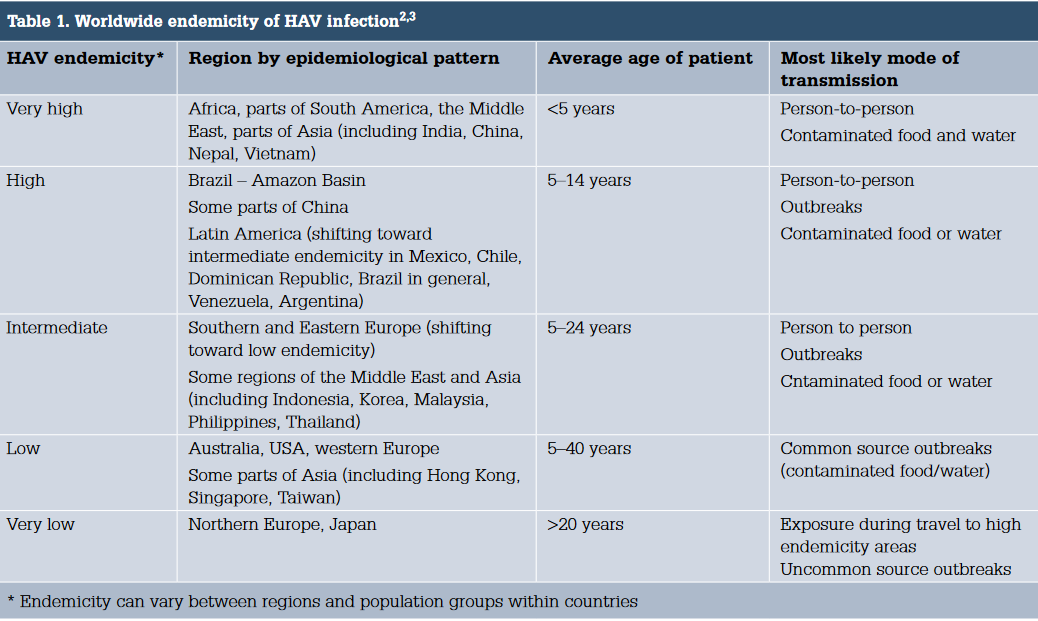
Global Patterns of Hepatitis A Epidemiology

- Groups Based on Endemicity:
- High Endemicity: Most children infected early, with few clinical diseases.
- Intermediate Endemicity: Higher incidence of sporadic cases and outbreaks among adolescents and young adults.
- Low Endemicity: Infections occur in specific settings or during travel.
- Shifts in Endemicity: Many regions transitioning from high to intermediate or low endemicity, increasing susceptibility among young adults.
- Global Case Increase: Estimated cases rose from 117 million in 1990 to 126 million in 2005.
Situation in Australia
- Endemicity Shift: Transitioned from intermediate to low endemicity since the 1950s.
- Seropositivity: By mid-1990s, 1–2% of 20-year-olds seropositive, increasing to 50% in those over 50 years.
- Immunity Trends: Naturally acquired immunity expected to decline further; many immune adults had asymptomatic infections in childhood.
- High Infection Rates in Specific Populations: Over 90% infection rates by age 5 in remote Aboriginal communities.
- Recent Outbreaks: Linked to faecally contaminated foods like oysters and semi-dried tomatoes, and in MSM and drug user communities.
Clinical
- Childhood infection is generally asymptomatic, while 75% of adults develop icteric disease
- Viral prodrome – fever, malaise, anorexia, headache, nausea
- Acute hepatitis then manifests
- dark urine
- followed by jaundice and pale stools 1–2 days later
- with gradual resolution of the other symptoms
- malaise and anorexia may persist and hepatic discomfort and pruritus may occur
- Hepatomegaly, splenomegaly
- liver function usually returns to normal or near normal within a month.
- complications are unusual but rarely include fulminant hepatitis.
- chronic infection does not occur, although 10% have prolonged or relapsing
- symptoms over 6–9 months
Investigations
- AST, ALT, bilirubin- Raised in acute hepatitis
- Anti HAV IgM detected early, perists 3-6 months
- IgG persists for life
Treatment
- Supportive – majority complete recovery
- Avoid hepatoxics – alcohol, paracetamol, low fat
- Outpatient if no coaguloapthy
- Very rarely fulminant and need liver transplant – Increased risk age and other chronic liver disease
Prevention
- Hygiene
- Avoid sharing personal items
- Don’t prepare food/drink for others
- Exclude from childcare/work – must be excluded from work for at least 1 week after the onset of jaundice.
- Notifiable condition
- Consider giving HAV vaccination or pre-exposure prophylaxis to suspectible contacts
- Contact trace back 50 days, infective from 2 weeks before jaundice to 1 week after
- No sexual contact for 1 week after jaundice
- Risk to travelers
- the risk to nonimmune travellers was considered to be 3/1000 per month of travel to a developing country in good quality accommodation
- 20/1000 per month for budget travellers including backpackers and trekkers
Vaccination
- Hepatitis A is the second most common vaccine preventable infection in travellers, influenza being most common,1 and the most common form of viral hepatitis.
- Single Dose Protection: A single vaccine dose can provide effective protection for several years, although a second dose is ideal.
- Delayed Doses: Effective immune response observed even when the second dose is delayed up to 6 years; doses given are valid regardless of delay.
- Last-Minute Travellers: It is clear that HA vaccine alone can be used for travellers right up to the day of departure, as there is strong evidence that vaccine works right up to and even up to 2 weeks after exposure.
- Interchangeability: Vaccines from different manufacturers are considered equivalent and interchangeable.
- Anti-HA IgM Detection: May be detectable in standard assays if tested within the first few weeks post-immunization, typically for diagnosing acute infection.
- Available Vaccines:
- Havrix (GlaxoSmithKline): Contains HM175 strain isolated from a case in Melbourne. Available as Havrix 1440 (1 mL, 1440 ELISA units) and Havrix Junior (0.5 mL, 720 ELISA units).
- Vaqta (Merck Sharp & Dohme): Based on the CR326F strain from Costa Rica. Adult dose contains 50 units (1 mL), pediatric/adolescent dose contains 25 units (0.5 mL).
- Avaxim (Sanofi-Aventis): Contains the GBM strain, each 0.5 mL dose containing 160 ELISA units, same dose for adults and children in Australia.
- Seroconversion:
- Rapid, with 88–96% seropositivity 2 weeks after a dose of Havrix.
- 98% seropositivity 2 weeks after a dose of Vaqta.
- contraindications
- history of anaphylaxis to a previous dose of hAV vaccine, or anaphylaxis to any of their components. combination hepatitis A/b
- history of anaphylaxis to yeast exists.
- Pregnancy is not a contraindication
- Target groups
- ATSI in NT, Qld, SA, WA
- Medical risk factors e.g. Chronic liver disease
- Ocupations – childcare, plumbers, sewage
- Travelling to endemic areas
- MSM and sex workers, IVDU, incarcerated
- Adverse Events from Hepatitis A Vaccination
- Local Reactions
- Prevalence: About 50% of adults and 20% of children experience local reactions.
- Symptoms: Injection site pain, redness, induration, and swelling.
- Duration: Most symptoms are mild and resolve within 1-2 days.
- Systemic Reactions
- Headache: Occurs in about 15% of adults, less commonly in children.
- Other Symptoms: Malaise, fatigue, fever, and nausea reported by approximately 5% of adult recipients.
- Characteristics: These systemic reactions are generally mild and short-lived.
- Serious Adverse Events
- Incidence: No increase in hematological, immunological, or neurological events (e.g., Guillain-Barré syndrome, brachial plexus neuropathy) compared to the unimmunized population.
- Safety Profile: Hepatitis A vaccines have not been associated with any serious adverse events, even in immunocompromised individuals.
- Local Reactions
- Contraindications
- Anaphylaxis: Restricted to individuals who have previously experienced anaphylaxis to a component of the HA vaccine or to a prior dose of the vaccine.
- Precautions
- Immunocompromised Persons
- Safety: The vaccine is safe for use in immunocompromised individuals, including those with HIV.
- Efficacy: May be less immunogenic in HIV-positive individuals, particularly if they have low CD4+ T-cell counts.
- Adverse Events: No increase in adverse events among those already immune to HA.
- Pregnancy
- Safety Assessment: The vaccine’s safety in pregnancy hasn’t been specifically assessed.
- Risk Considerations: As the vaccine uses inactivated HA, no risk to the fetus or mother is expected.
- Official Stance: ATAGI does not consider pregnancy or breastfeeding as contraindications to HA immunization.
- Children
- Safety and Efficacy: Safe and immunogenic in children.
- Age Limits:
- Vaqta: Approved for use from 1 year of age.
- Avaxim and Havrix: Approved for use from 2 years of age, though Havrix is inconsistently approved for Twinrix from 1 year.
- Vaccine Use in Infants:
- Extensively evaluated and shown to be well-tolerated and immunogenic.
- Antibody Titre: Reduced in infants of HA seropositive mothers, but seroconversion and immune priming remain effective.
- Additional Doses: Interference from maternally derived antibodies can be managed by an additional vaccine dose in the second year of life.
- General Recommendation: Comfortable with use from 12 months of age; routine immunization typically starts at 12 months in various regions, including parts of Australia and the USA.
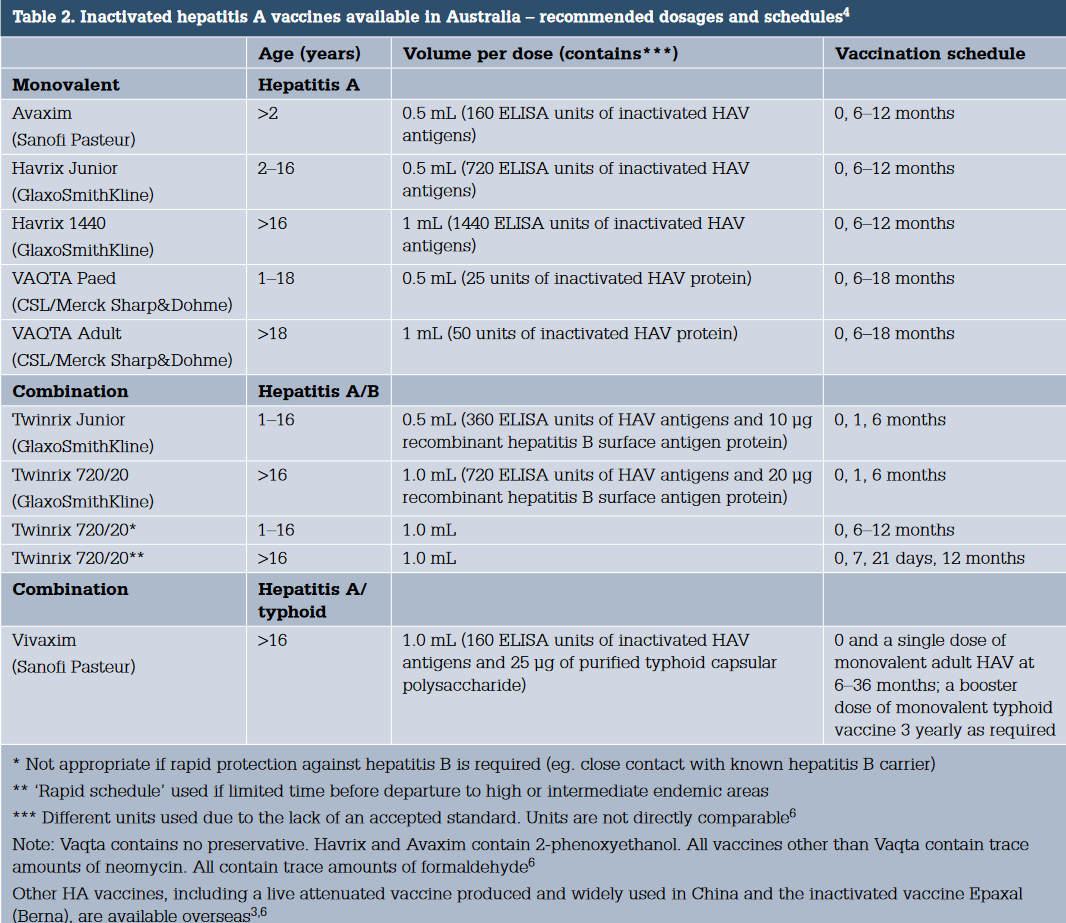
Combined Hepatitis A and B Immunization: Twinrix (GlaxoSmithKline)
- Vaccine Composition: Contains inactivated hepatitis A virus and genetically engineered hepatitis B surface antigen (HBsAg).
- Formulations:
- Twinrix Adult: Volume: 1 mL dose. HA content: 720 ELISA units. HBsAg content: 20 μg of recombinant protein.
- Twinrix Junior: Volume: 0.5 mL dose. HA content: 360 ELISA units. HBsAg content: 10 μg of recombinant protein.
- Vaccine Components: Identical to those used in their respective monovalent vaccines produced by the same manufacturer.
Schedule:
- Standard: Three doses at 0, 1, and 6 months.
- Rapid Schedule: Doses at 0, 7, and 21 days with a booster at 12 months, suitable for travelers needing quick protection.
- Children and Adolescents:
- Alternative Schedule: Two-dose schedule using the 720/20 formulation; not suitable for immediate protection against hepatitis B.
Recommendations:
HA-HB vaccine is recommended for those at risk of both infections, including:
- Travellers to areas of moderate and high prevalence of HA and HB
- Medical, dental, nursing and other health professional students
- Aboriginal and Torres Strait Islander children living in NT, Queensland, SA and
WA and those who regularly provide care for them - People who have anal intercourse, including men who have sex with men and
commercial sex workers - People who inject drugs
- Patients with chronic liver disease, particularly hepatitis C
- People with developmental disabilities and their carers
- Inmates of correctional facilities
- Military personnel